 |
| PneumoDart® Kit (Aguja/Catéter) de DESCOMPRESIÓN NEUMOTÓRAX |
{kind=link}
Les Esperamos en Grupo en TELEGRAM
de Emergencias https://t.me/joinchat/GRsTvEHYjNLP8yc6gPXQ9Q
El PneumoDart es una solución fiable para el tratamiento de un neumotórax de tensión. Desarrollada de acuerdo con las directrices del TCCC con el Departamento de Defensa de los EE.UU.
Ofrece una mayor eficiencia y seguridad.
Los métodos actuales para el tratamiento del pneumotórax requieren la aplicación de un sello sobre el pecho e insertar el catéter para facilitar el drenaje. Sin embargo, la aplicación con éxito de una aguja neumotórax tradicional ha demostrado ser difícil.
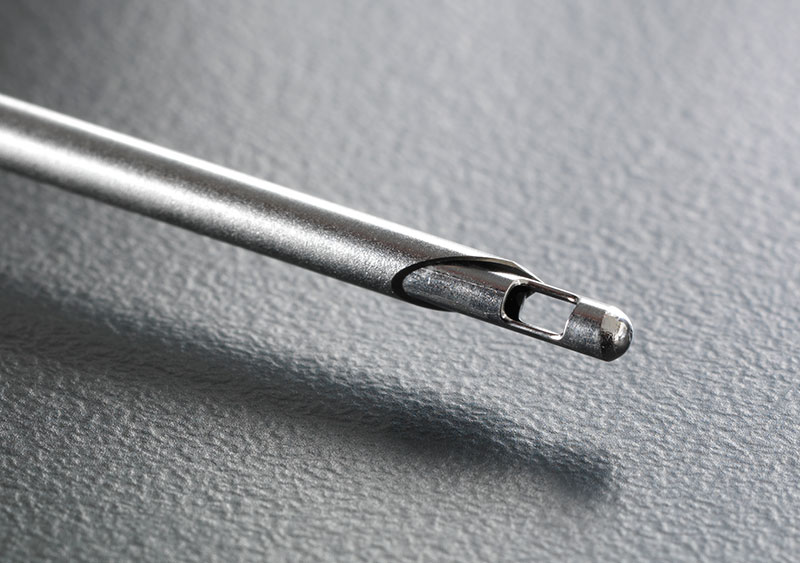
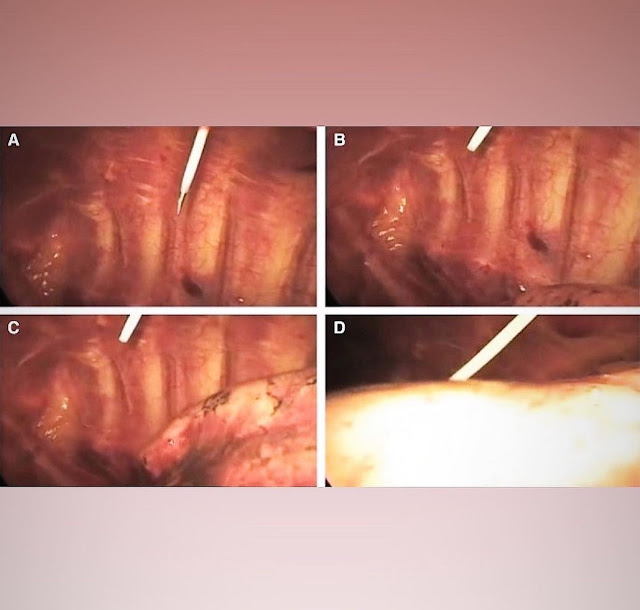
El PneumoDart tiene una punta de seguridad que reduce el riesgo de punción de los órganos internos cuando se inserta.
Cabeza transparente que permite monitorizar el aire o la sangre que sale del pecho.

Description:
The PneumoDart is a reliable solution for treating a tension pneumothorax injury, or sucking chest wound. Our robust innovation helps you to get it right, first time.
It offers better efficiency, safety and important physical features. Typical methods for treating this kind of injury include the application of a plastic seal over the chest wound to inserting a needle catheter into the chest to drain air out of the chest and relieve pressure. However, successful application of a traditional pneumothorax needle has proven difficult.
Our needle is 3.25” which is the optimal length as recommended by the Tactical Combat Casualty Care (TCCC) who inspired the PneumoDart and we developed it with the US Department of Defense during a robust testing and evaluation phase.
Details:
- 14ga x 3.25”
- Veress safety tip to reduce the risk of puncturing internal organs when inserted.
- Visible cap head to monitor air or blood leaving the chest.
- Luer lock cap allows for an active drawing or elimination of air or blood from the chest.
- Seven year shelf life
- NSN 6515-01-655-9514 and CE marked.
 |
| PNEUMODART KIT DESCOMPRESIÓN NEUMOTÓRAX PneumoDart® |
 |
| PNEUMODART KIT DESCOMPRESIÓN NEUMOTÓRAX PneumoDart® |
 |
| PNEUMODART KIT DESCOMPRESIÓN NEUMOTÓRAX PneumoDart® |
 |
| PNEUMODART KIT DESCOMPRESIÓN NEUMOTÓRAX PneumoDart® |
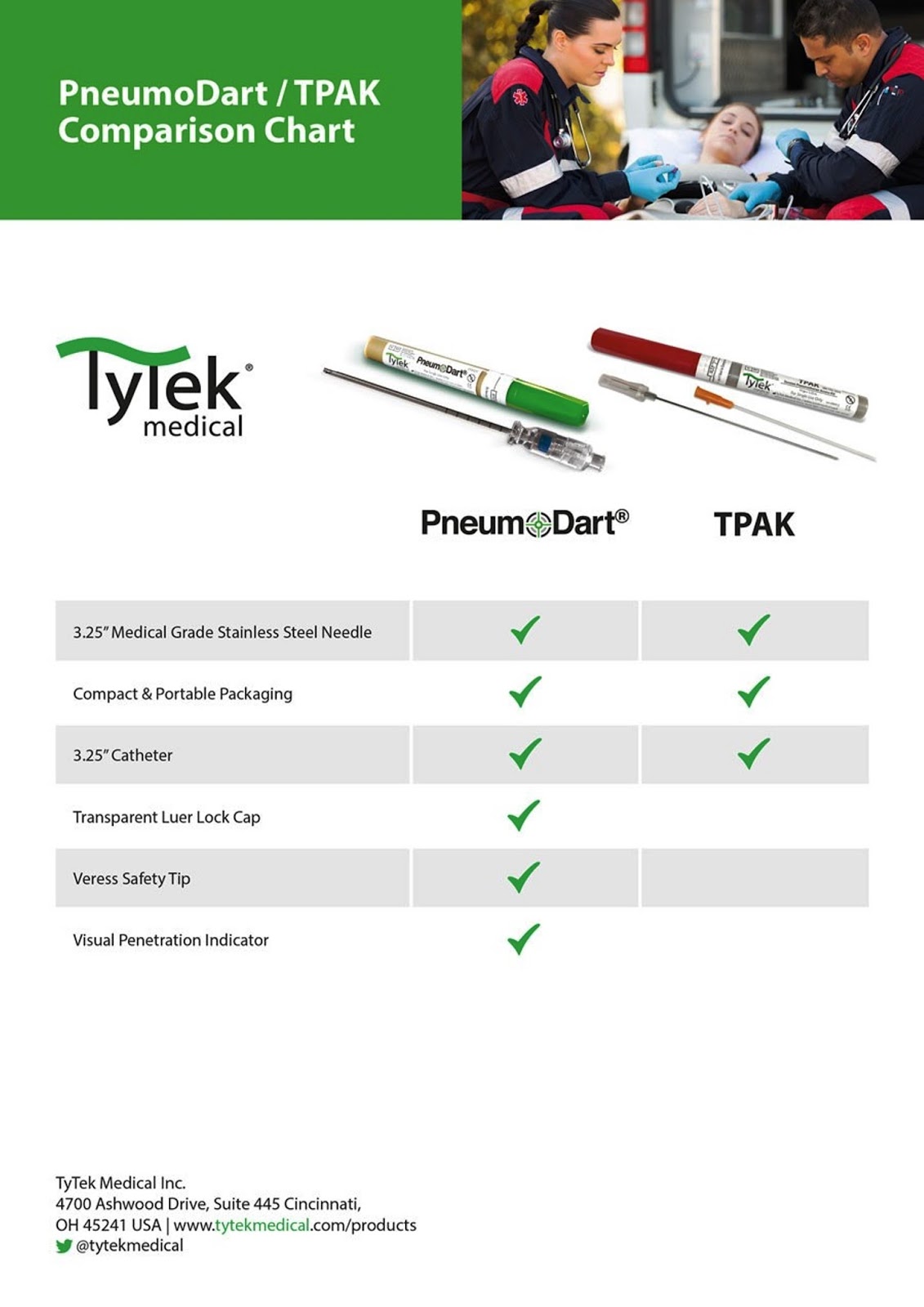
Pneumodart vs TyTek
Dr. Ramon Reyes, MD
#McTAC #MEDICO #MD #MedicalDoctor #TACMEDSpain #EMS #TacticalMedicalSpecialist #TCCC #TECC #TACMED #TCCCac #TCCCmp #TCCLEFR #EMS
Sorprendente por @the.prehospitalist AGUJA D: habilidad rápida y salvavidas para el neumo a tensión.
🫁CRITERIOS:
•Neumo a TENSIÓN, no neumo simple (abierto o cerrado)
• Sonidos pulmonares ausentes o gravemente disminuidos MÁS inestabilidad hemodinámica (signos de hipoperfusión)
•Otros indicadores = JVD, taquicardia, hipoxia, dolor torácico, etc.; sin embargo, LS ausente/severamente disminuido en presencia de hipoperfusión = indicador principal
•Descompresión bilateral en paro traumático factible
HITOS:
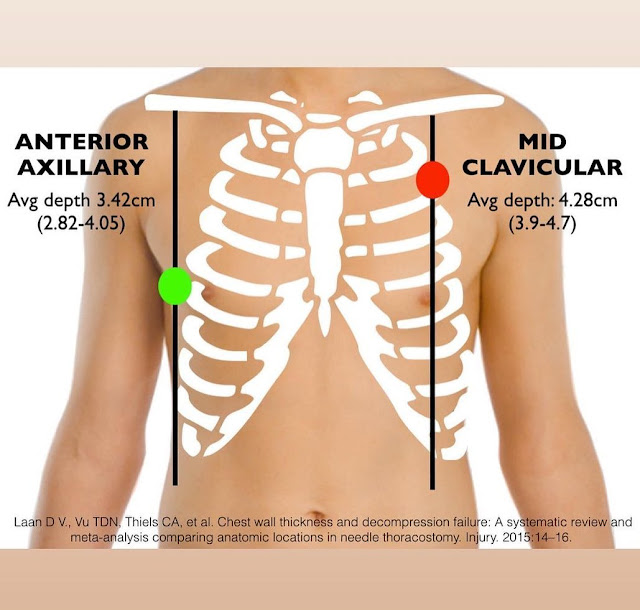
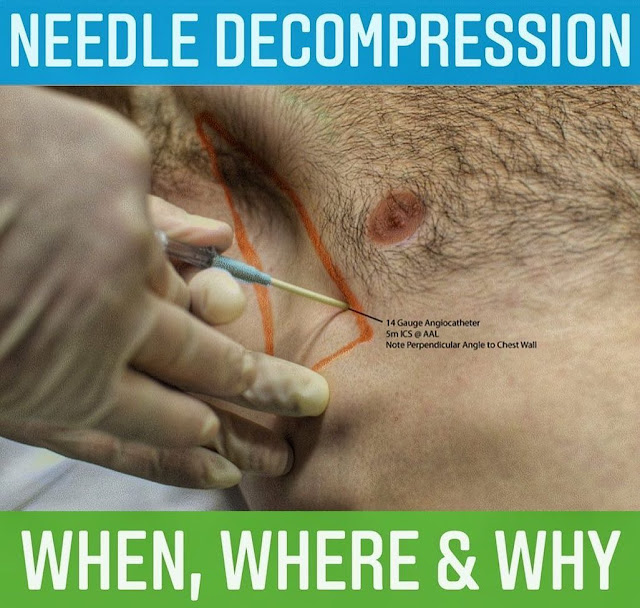
1️⃣Línea axilar anterior, 4º-5º ICS
•Hombres: trazar la línea del pezón hasta AAL y lanzar
•Mujeres/pacientes con tejido mamario: trace el pliegue inframamario y suba un ICS
2️⃣Medio-clavicular, 2do ICS
•La clavícula se extiende hasta la punta del hombro; "clavicular medio" es más lateral de lo que se piensa a menudo
•Considere la clavícula como la primera costilla (está debajo). El espacio a continuación es el 1er ICS. Baja un espacio más y listo.
• Si es posible, vaya por encima de las costillas en lugar de por debajo para evitar los nervios y los vasos sanguíneos que corren por debajo.
🧐PACIENTES FLUFFY: Las costillas no siempre son fácilmente palpables. Calcule el área apropiada e inserte la aguja. Si se alcanza la costilla, simplemente gire la aguja hacia arriba y por encima.
COMPLICACIONES:
•Metiendo corazón o grandes vasos ♀️
• Pinchar el hígado, el bazo, el diafragma o el parénquima pulmonar
• Aguja demasiado corta para alcanzar el espacio pleural
• Catéter torcido u obstruido
•Causar neumo si uno no estaba realmente presente
🥸IMITADOR:
•Las contusiones pulmonares pueden simular una tensión con LS triste e inestabilidad hemodinámica. Tratar por neumo si está justificado, pero considerar contusiones si no hay mejoría e hipoxia refractaria.
AGUJA V. DEDO:
•¿Todavía hay lugar para la aguja D si está disponible la toracostomía con el dedo?
•SÍ. Es rápido y, a menudo, efectivo para aliviar la amenaza inmediata de la vida. Muchas situaciones prehospitalarias en las que un dardo es la medida de primera línea adecuada, seguida de una toracostomía digital si es refractaria.
☠️PARO CARDÍACO:
•La CA traumática no se resuelve con RCP/epi. Priorizar intervenciones como dardos bilaterales.
⚠️: A veces nos equivocamos con DDx. Ser capaz de justificar acciones y ser responsable en la señalización para evitar complicaciones innecesarias. El riesgo de pasar por alto una tensión en un paciente que lo parece es mucho peor que causar un pequeño neumo iatrogénico.
Amazing by @the.prehospitalist NEEDLE D: rapid & life-saving skill for tension pneumo.
🫁CRITERIA:
•TENSION pneumo, not simple pneumo (open or closed)
•Absent or severely diminished lung sounds PLUS hemodynamic instability (signs of hypoperfusion)
•Other indicators = JVD, tachycardia, hypoxia, chest pain, etc.; however, absent/severely diminished LS in presence of hypoperfusion = major indicator
•Bilateral decompression in workable traumatic arrest
LANDMARKS:
1️⃣Anterior axillary line, 4th-5th ICS
•Males - trace nipple line over to AAL and dart
•Females/patients with breast tissue - trace inframammary fold over and go up one ICS
2️⃣Mid-clavicular, 2nd ICS
•Clavicle extends to tip of shoulder; “mid-clavicular” is more lateral than often thought
•Consider the clavicle the first rib (it’s underneath). Gap below is 1st ICS. Go down one more space and voilà.
•Go above rather than below rib if possible to avoid nerves and vessels that run underneath.
🧐FLUFFY PATIENTS: Ribs are not always easily palpable. Estimate appropriate area and insert needle. If rib is met, simply rotate needle upward and over.
COMPLICATIONS:
•Poking heart or great vessels ♀️
•Poking liver, spleen, diaphragm or lung parenchyma
•Needle too short to reach pleural space
•Catheter kink or clog
•Causing pneumo if one wasn’t actually present
🥸MIMICKER:
•Pulmonary contusions can closely mimic a tension with sad LS and hemodynamic instability. Treat for pneumo if justified, but consider contusions if no improvement and refractory hypoxia.
NEEDLE V. FINGER:
•Is there still a place for needle D if finger thoracostomy is available?
•YES. It’s fast af boi and often effective at relieving immediate life-threat. Many prehospital situations where a dart is appropriate first-line measure, followed by finger thoracostomy if refractory.
☠️CARDIAC ARREST:
•Traumatic CA is not solved by CPR/epi. Prioritize interventions like bilateral darts.
⚠️: Sometimes we’ll be wrong about DDx. Be able to justify actions and be responsible about landmarking to avoid unnecessary complications. Risk of missing a tension in a patient who looks like one is far worse than causing a small iatrogenic pneumo.
Trauma de Tórax, ver y compartir vía Facebook https://www.facebook.com/photo/?fbid=774562247373195&set=pb.100044582790771.-2207520000.
Dr Ramon REYES, MD,
Por favor compartir nuestras REDES SOCIALES @DrRamonReyesMD, así podremos llegar a mas personas y estos se beneficiarán de la disponibilidad de estos documentos, pdf, e-book, gratuitos y legales..
Grupo Biblioteca/PDFs gratis en Facebook
https://www.facebook.com/groups/PDFgratisMedicina #DrRamonReyesMD
https://www.facebook.com/DrRamonReyesMD
https://www.instagram.com/drramonreyesmd/
https://www.pinterest.es/DrRamonReyesMD/
https://twitter.com/eeiispain
Blog
http://emssolutionsint.blogspot.com/2016/12/dr-ramon-reyes-diaz-md-emt-t-dmo.html
TELEGRAM
Group https://t.me/joinchat/GRsTvEHYjNLP8yc6gPXQ9Q