
 Background: Upper endoscopy allows for the identification of the source of bleeding as well as hemostatic treatment for actively bleeding lesions In patients with upper gastrointestinal bleeding (UGIB). Definitive treatment with endoscopic hemostatic treatment can potentially stop bleeding in high-risk lesions and reduce further bleeding and the need for surgery. The optimal time for endoscopy to be performed is unknown. The definition of urgent varies depending on which study you read, ranging from 2 hours up to 12 hours. Additionally, most previous studies only enrolled patients who were not hemodynamically unstable or high-risk, which is frequently what we are dealing with in the emergency department.
Background: Upper endoscopy allows for the identification of the source of bleeding as well as hemostatic treatment for actively bleeding lesions In patients with upper gastrointestinal bleeding (UGIB). Definitive treatment with endoscopic hemostatic treatment can potentially stop bleeding in high-risk lesions and reduce further bleeding and the need for surgery. The optimal time for endoscopy to be performed is unknown. The definition of urgent varies depending on which study you read, ranging from 2 hours up to 12 hours. Additionally, most previous studies only enrolled patients who were not hemodynamically unstable or high-risk, which is frequently what we are dealing with in the emergency department.
The Glasgow-Blatchford score is a validated risk-assessment score for the prediction of clinical outcomes, including the need for intervention and risk of death. The score ranges from 0 to 23, with higher scores indicting a higher risk of further bleeding or death. A threshold score of ≥7 has been shown to be the most accurate predictor of whether a patient will need endoscopic treatment.2 There are conflicting results regarding urgent endoscopy (within 6 hours after admission) and mortality.
REBEL Cast Episode 82 – Timing of Endoscopy for UGIB
Paper: Lau JYW et al. Timing of Endoscopy for Acute Upper Gastrointestinal Bleeding. NEJM 2020. PMID: 32242355
Clinical Question: In patients admitted with acute UGIB who are predicted to be at high risk (Glasgow-Blatchford score ≥12) for further bleeding or death, does endoscopy performed within 6 hours after gastroenterologic consultation (urgent endoscopy) or endoscopy performed between 6 to 24 hours after consultation (early endoscopy) decrease further bleeding and improve outcomes?
What They Did:
- Randomized clinical trial
- Patients assigned in a 1:1 ratio
- Urgent Endoscopy = Endoscopy within 6 hours after consultation
- Early Endoscopy = Endoscopy the next morning and within 24 hours after consultation
- Emergency endoscopy was offered if there were signs of further bleeding (i.e. fresh hematemesis or hematochezia, hypotensive shock, or both)
- Standard medical therapy provided to all patients:
- Both groups received IV high-dose infusion of proton pump inhibitor (80mg bolus, followed by 8mg/hr) on admission
- Patients with suspected variceal bleeding (i.e. known liver disease, stigmata of liver cirrhosis, or a history of bleeding esophagogastric varices) received vasoactive drugs as well as IV antibiotics
Outcomes:
- Primary: Death from any cause within 30d after randomization
-
Secondary:
- Receipt of endoscopic therapy at 1st endoscopy
- Further bleeding (persistent or recurrent bleeding)
- Hospital LOS
- ICU LOS
- Receipt of further endoscopic treatment
- Emergency surgery or angiographic embolization to achieve hemostasis
- Blood transfusions
- Adverse events within 30d after randomization
Inclusion:
- Age ≥18 years
- Patients with overt signs of acute UGIB (hematemesis, melena, or both)
- Predicted to be high risk for further bleeding or death (Glasgow-Blatchford score of ≥12) [See Discussion]
Exclusion:
- Age <18 years
- Unable to provide informed consent
- Pregnancy
- Moribund from terminal illness
- Hypotensive shock
- Condition did not stabilize after initial resuscitation
Results:
- 516 patients enrolled
- Screened 4,715 patients with acute UGIB and only 598 had Glasgow-Blatchford score of ≥12
- Peptic ulcers were the source of bleeding in ≈62% of patients
- Emergency endoscopy was performed in 20 patients (7.8%) in the early endoscopy group due to new onset signs of bleeding (11 patients for hypotension, 6 patients for fresh hematemesis, 2 patients for fresh melena, 1patient for substantial decrease in hemoglobin)
Critical Results:
-
No difference in:
- Patients who underwent surgery or angiographic treatment between groups
- Hospital LOS or need for ICU admission
- Percentage of patients who required blood transfusion or number of units transfused (≈90% and 2.4 units respectively)
- Post-hoc analysis also showed no difference according to the time of day and patients with further bleeding and death
Strengths:
- Randomized clinical trial
- Useda hard, patient centered outcome of death at 30 days from any cause
- Asks a clinically important question in an area with limited available data
- Investigates the right subset of patients (i.e. not those that are really sick and not those that will clearly be fine no matter what)
- No data was missing from the intention-to-treat analysis
- Used a validated Glasgow-Blatchford score to assess risk of further bleeding and death
Limitations:
- Confidence intervals of the secondary outcomes were not adjusted for multiple comparisons and there for hypothesis generating
- In the urgent endoscopy group 48.1% of patients underwent endoscopy in the 6 to 12-hour window.
- Patients in the urgent endoscopy group had slightly more comorbid conditions (i.e. Ischemic heart disease, cancer, renal disease, and liver cirrhosis) which could bias the results of the study favoring early endoscopy
- The proportion of patients with variceal bleeding in this study was small and therefore the findings of this trial may not be applicable places where you see a higher percentage of varices (i.e. inner-city populations, liver transplant centers, etc…)
Discussion:
- Mean time from GI consultation to endoscopy was 2.5 +/- 1.7hrs in the urgent endoscopy group vs 16.8 +/- 6.8hrs in the early endoscopy group. Mean time from presentation to endoscopy was 9.9 +/- 6.1hrs in urgent endoscopy vs 24.7 +/- 9.0hrs in the early endoscopy groups. In a disease that has up to a 9% mortality rate, maybe “early”, should truly mean “early”. Why not compare endoscopy within 6hrs to within 2hrs?
- 8% of patients who were thought to be “stable for entry into the study decompensated and needed emergency endoscopy (cross over rate was 7.8%). This shows how quickly these patients can get sick. What this should mean is that in all patients with significant GIB who you classify as high risk should have emergency consultation with GI and consideration for immediate/early endoscopy or at least, ICU admission for close monitoring. If you don’t work in a hospital with GI available, these patients should be transferred to a facility that does.
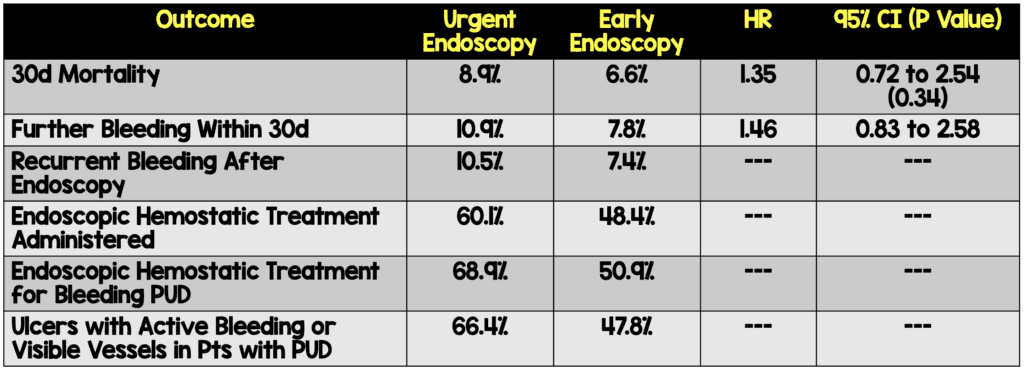
- Since the sickest patients (HD unstable) are not included in this study, the observed mortality rate in this study is rather low (≈6.6 to 8.9%), but it should be high enough for us to detect differences in mortality in patients with high Glasgow Blatchford scores outcomes
- The authors of this paper picked a Glasgow Blatchford score of ≥12 to define high risk. The risk of needing a procedure or risk of mortality gradually increase as the score gets higher. A score of ≥12 seems to be based off a single observational study done in 2011 [3]. I am not sure that a score ≥12 vs ≥7 predicts a higher mortality or need for intervention more accurately (i.e. 12 isn’t more accurate than 7 based on best available data)
- Endoscopy was performed between 6pm and 5:59am in 37.6% of patients in the urgent endoscopy group and 6.7% of the early endoscopy group
- This was not a very sick group of patients included in this study:
- SBP ≈108mmHg (SBP <90mmHg ≈15% of patients)
- HR >100BPM ≈34% of patients
- Hemoglobin Level on Admission ≈7.3g/dL
- IMPORTANT NOTE: This study does not apply to the crashing or hemodynamically unstable UGIB patient. The authors excluded patients with hemodynamic instability, which is the patient population we are most concerned about in the ED. To quote the authors: “Our results are not generalizable to patients with ongoing bleeding and hypotensive shock, who require urgent intervention.”
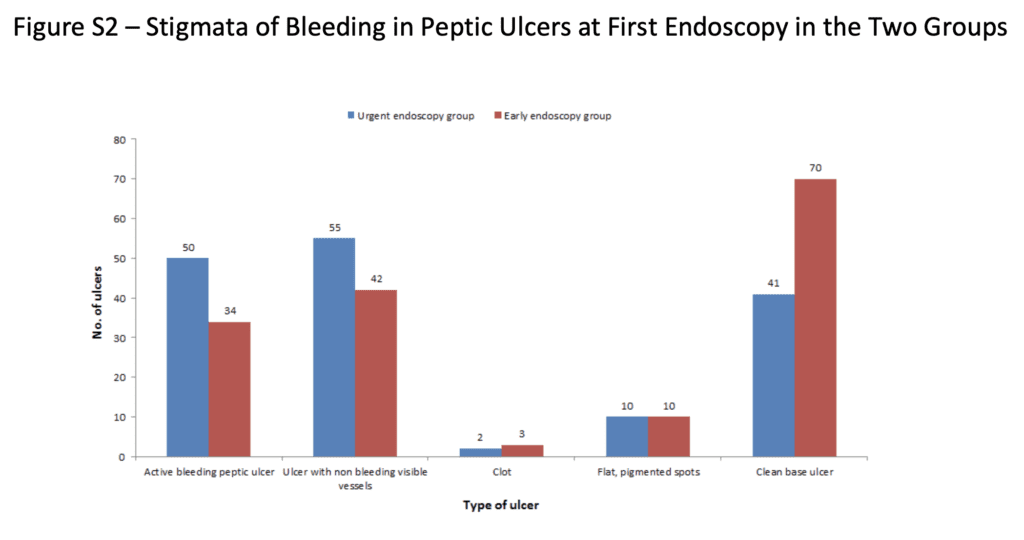
- The authors point out that there were numerically more deaths in the urgent-endoscopy group and raise the possibility that patients may benefit from treatment for coexisting medical illnesses and a period of acid suppression. This is true in patients with who are hemodynamically stable…optimize all medical conditions and perform delayed endoscopy. This can be seen when looking at the stigmata of bleeding in patients with PUD and endoscopy (Patients with medical treatment had less stigmata of bleeding)
- In patients who are hemodynamically unstable the first priority is adequate resuscitation. Some patient will stabilize and can be admitted to the ICU for sooner rather than later endoscopy. However, in non-responders or transient responders, despite maximal resuscitation and medical therapy, the optimal time for endoscopy is likely as soon as possible (ASAP). It is no surprise that sicker patients typically get earlier endoscopy but do worse. This is simply because they are just sicker. There is no real clinical or physiological reason why these patients would become more unstable during endoscopy. (I highly recommend you listen to REBEL Cast Ep36, where this is discussed).
- My workflow is below:
- All UGIB patients = consult GI immediately
- Timing of Endoscopy:
- In patients are HD unstable at any time = push for early (meaning immediate endoscopy) while resuscitation is ongoing
- In patients who are not HD unstable at any point, do a Glasgow Blatchford score and if ≥7 = push for ICU admission
- In patients who are not HD unstable at any point, do a Glasgow Blatchford score and if <7 = consider telemetry/floor admission
Author Conclusion: “In patients with acute upper gastrointestinal bleeding who were at high risk for further bleeding or death, endoscopy performed within 6 hours after gastroenterologic consultation was not associated with lower 30-day mortality than endoscopy performed between 6 and 24 hours after consultation.”
Clinical Take Home Point: In this RCT of patients with UGIB in patients who are HD stable at high risk of bleeding, this study does not answer the question of <6hrs vs 6 – 24hrs for timing of endoscopy as only ¼ of patients had endoscopy at <6hours. In patients who are hemodynamically unstable (mostly excluded in this study), who are receiving maximal resuscitation and medical therapy and non-responders or transient responders, the optimal time for endoscopy is likely as soon as possible (ASAP).
References:
- Lau JYW et al. Timing of Endoscopy for Acute Upper Gastrointestinal Bleeding. NEJM 2020. PMID: 32242355
- Stanley AJ et al. Comparison of Risk Scoring Systems for Patients Presenting With Upper Gastrointestinal Bleeding: International Multicentre Prospective Study. BMJ 2017. PMID: 28053181
- Lim LG et al. Urgent Endoscopy is Associated with Lower Mortality in High-Risk But Not Low-Risk Nonvariceal Upper Gastrointestinal Bleeding. Endoscopy 2011. PMID: 21360421
For More Thoughts on This Topic Checkout:
- REBEL Cast: Ep36 – Resuscitate Before You Endoscopate?
- The Bottom Line: Timing of Endoscopy for Acute Upper Gastrointestinal Bleeding
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)


The post REBEL Cast Ep82: Timing of Endoscopy for UGIB appeared first on REBEL EM - Emergency Medicine Blog.