
Take Home Points
- Acute closed angle glaucoma is an ophthalmologic emergency that usually presents with sudden, painful, monocular vision loss.
- Physical exam will reveal conjunctival redness, corneal haziness or cloudiness due to edema and a pupil that is mid sized and minimally reactive to light, a rock hard globe and IOP >/= 21.
- These patients require emergent ophthalmology evaluation but treatment should be started empirically while waiting for the evaluation. Initial treatment to decrease IOP usually includes a topical BB such as timolol and topical AB such as apraclonidine and either IV or PO acetazolamide.
REBEL Core Cast 19.0 – Acute Angle Closure Glaucoma
Click here for Direct Download of Podcast
Show Notes
 What is it?
What is it?
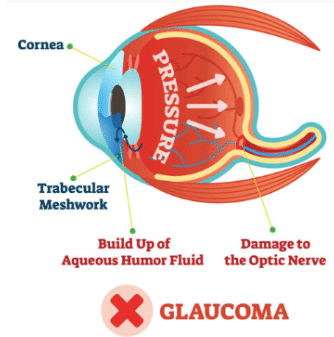
- Group of diseases that have increased intraocular pressure (IOP) causing optic nerve damage leading to decreased vision
-
Different types of glaucoma
- Open-angle glaucoma
- Closed-angle glaucoma
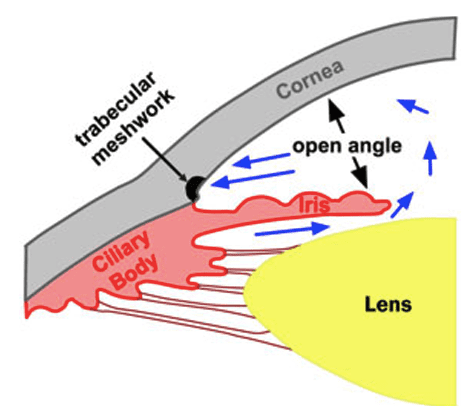
Open-Angle Glaucoma
- Most common type
- Characteristized by progressive peripheral visual field loss followed by central
- Likely because of increased resistance to aqueous outflow through trabecular meshwork
- Patients generally have increased IOP
Closed-Angle Glaucoma
- Worrisome pathology in the emergency department
- Closing / Narrowing of the anterior chamber angle
- Increased aqueous humor collection leads to increased IOP and damage to the optic nerve
- Presents with sudden painful vision loss, red eye, halos, frontal or supraorbital headache
 Differential for Painful Red Eye
Differential for Painful Red Eye
- Corneal abrasion
- Conjunctivitis
- Subconjunctival hemorrhage
- Iritis
- Episcleritis
- Infectious keratitis
- Traumatic hyphema
Risk Factors for Glaucoma
- Family history
- Age >60 years
- Female Gender
- Far sighted
- Medications (HCTZ, albuterol, SSRI, TMP-SMX among others)
- Inuit & Asian ethnicity
Eye Exam
- Any person presenting with vision loss or eye pain deserves full exam
- Visual acuity
- Pupil exam
- Visual field testing
- Evaluation of IOP with a tono-pen
- Slit-lamp exam
- Fundoscopy
Physical Exam
- Conjunctival redness
- Corneal haziness
- Mid sized pupil minimally reactive to light
-
Palpate eye – potentially “rock hard”
- Always use the tono-pen , >20 IOP
Treatment
- Consult ophthalmology
- Topical beta blocker – timolol
- Topical alpha agonist – Apraclonidine
- 500 mg IV / PO acetazolamide
- Recheck IOP hourly, keep head in supine position, keep in bright room
For More on This Topic Checkout:
- Core EM: Non-Traumatic Monocular Vision Loss
- WikEM: Acute angle-closure glaucoma
- WikEM: Tono-Pen Use
Shownotes Written By: Miguel Reyes, MD (Twitter: @miguel_reyesMD)
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post REBEL Core Cast 19.0 – Acute Angle Closure Glaucoma appeared first on REBEL EM - Emergency Medicine Blog.