 Background: Stress related gastrointestinal mucosal damage is a commonly encountered problem in the critically ill patients admitted to the intensive care unit. The incidence ranges from 0.6-7% and is decreasing partly due to aggressive resuscitation strategies and focus on early enteral feeding1. Damage to the mucosal integrity occurs in conditions associated with increased inflammation and reduced mucosal perfusion 2. Despite its decreasing incidence, stress related GI bleed remains a major challenge for the intensivist with many studies showing increase in mortality and ICU length of stay in these patients3.
Background: Stress related gastrointestinal mucosal damage is a commonly encountered problem in the critically ill patients admitted to the intensive care unit. The incidence ranges from 0.6-7% and is decreasing partly due to aggressive resuscitation strategies and focus on early enteral feeding1. Damage to the mucosal integrity occurs in conditions associated with increased inflammation and reduced mucosal perfusion 2. Despite its decreasing incidence, stress related GI bleed remains a major challenge for the intensivist with many studies showing increase in mortality and ICU length of stay in these patients3.
Stress ulcer prophylaxis is recommended for critically ill patients at risk for GI bleed; the major risk factors include need for prolonged mechanical ventilation, coagulopathy, hepatic and renal failure. There is high quality evidence supporting the use of H2 receptor antagonists (H2RA) and proton pump inhibitors (PPI) in these patients. Many international surveys show that PPIs are currently preferred for acid suppression4. Though many randomized controlled trials support the use of PPI over other acid suppressants, there is clearly no recommendation regarding benefits of one group over the other. Alhazzani et al5recently published a network meta-analysis of 57 trials enrolling over 7000 patients that showed moderate quality evidence that PPIs are more effective than H2 blockers, sucralfate or placebo in preventing clinically significant GI bleed though there is a possible increase in risk for pneumonia with similar mortality. Another meta-analysis by Alshamsi et al showed that PPIs were more effective than H2RAs in reducing the risk of clinically important GI bleeding and overt GI bleeding without a significant increase in risk for pneumonia, mortality and ICU length of stay6
Furthermore, there is growing concern that acid suppression predisposes patients to increased risk for nosocomial infections like pneumonia and Clostridium difficile as well as cardiovascular events. This was demonstrated in a few randomized clinical trials as well as a few observational studies7,8. The authors of the current study aimed to evaluate the benefits and adverse events associated with the use of pantoprazole for stress ulcer prophylaxis in patients at risk for gastrointestinal bleeding9
Article: Krag Met al. Pantoprazole in patients at risk for gastrointestinal bleeding in the ICU. N Engl J Med2018;379:2199-2208. PMID: 30354950
Clinical Question: Does stress ulcer prophylaxis with pantoprazole reduce 90-day mortality when compared to placebo in critically ill patients admitted to the ICU with risk factors for GI bleed?
What They Did:
- Multicenter, stratified, parallel-group, placebo-controlled, blinded clinical trial
- 10,000 patients were initially assessed for eligibility. A total of 3298 patients were enrolled; 1645 were assigned to the pantoprazole and 1653 to the placebo group
- Patients from 33 ICUs in Denmark, Finland, the Netherlands, Norway, Switzerland, and the United Kingdom were enrolled in the study
- Patients in both groups had similar baseline characteristics except for chronic lung disease and coagulopathy which was higher in the intervention group. More patients in the placebo group needed emergency surgery
- Patients in both groups had similar requirement for invasive mechanical ventilation, renal replacement therapy and vasopressors. Median SAPS II and SOFAcores on admission were similar as well
- SOFA(Sequential Organ Failure Assessment) score ranges from 0 to 24 and is a morbidity and mortality prediction score based on dysfunction of six organ systems. A higher score predicts worse outcomes
- SAPS II(Simple Acute Physiology Score) ranges from 0 to 163 and is calculated from 17 physiologic variables with a higher score indicating more severe disease
- Intervention: IV Pantoprazole 40 mg daily as a single bolus vs matched placebo from randomization to 90 days or ICU discharge/death
- More than 99% of patients in both the groups were included in mortality and secondary outcome analyses
Inclusion Criteria:
All patients who were 18 years or older and acutely admitted to the ICU with one or more of the following risk factors for gastrointestinal bleeding:
- Shock (Systolic BP <90mm Hg/MAP <70mm Hg/continuous vasopressor use/lactate >4mmol/L)
- Acute or chronic intermittent or continuous renal replacement therapy
- Invasive mechanical ventilation which was expected to last more than 24 hours
- Coagulopathy (platelets <50 × 109/l or INR >1.5 or prothrombin time > 20 s)
- Ongoing treatment with anticoagulant drugs (prophylactic doses excluded)
- History of coagulopathy
- History of chronic liver disease
Exclusion Criteria:
- Contraindications to proton pump inhibitors or use of Atazanavir
- Ongoing treatment with PPI and/or H2-receptor antagonists on a daily basis
- Gastrointestinal bleeding of any origin
- Diagnosis of peptic ulcer during current hospital admission
- Organ transplant during current hospital admission
- Withdrawal from active therapy or brain death documented in the patient charts
- Pregnant women
- Consent according to national regulations not obtainable
Outcomes:
Primary Outcome:
- Death by 90 days after randomization
Secondary outcomes:
- Clinically important events in the ICU (Gastrointestinal bleeding, new-onset pneumonia, C. difficile infection, acute myocardial ischemia)
- Clinically important gastrointestinal bleeding in the ICUefined as overt GI bleeding (presence of hematemesis, blood tinged GI aspirate or melena) and at least one of the following four features within 24 hours of GI bleed:
- Spontaneous decrease in SBP, MAP or DBP ≥20mmHg
- Initiation of treatment with a vasopressor or a 20% increase in vasopressor dose
- Decrease in hemoglobin of at least 2g/dL
- Transfusion of two or more units of PRBCs
- Infectious adverse events in the ICU
- New-onset pneumonia
- New-onsetdifficileinfection
- Severe adverse reaction
- The percentage of days alive without the use of life support within the 90-day period
Results:
- Median length of stay in each group: 6 days
- Median number of days trial agent was administered in each group: 4 days
- Enteral feeds on day 1: 2% in the pantoprazole and 56.4% in the placebo group
- 85% of patients in both groups received enteral nutrition by day 5
Strengths:
- Trial was funded by Innovation Fund Denmark, but had no role in the design of the protocol, the trial conduct, the analysis, or reporting of data
- Trial group assignments were concealed from the patients, clinicians, investigators, trial statisticians, and members of the data and safety monitoring committee
- Large multicenter population of patients reflecting different practice patterns
- Patients in both groups had equally matched baseline characteristics
- Primary and secondary outcomes are clinically relevant in daily practice
- No major changes in practice apart from the planned intervention
- Allays fears associated with pantoprazole use
Limitations:
- The study was powered to detect a 5% difference in all-cause mortality for a population of 3,550 patients which the study did not reach as a large number of patients were excluded after initial enrollment
- ther interventions that could affect the primary outcome were chosen at the discretion of clinicians
- >130 patients in each group did not give consent or withdrew consent and >100 patients in each group had indications for open-label acid suppression lowering the overall number of patients randomized to each group
- There was no assessment of other medical interventions
- Absence of reported serious adverse reactions to pantoprazole suggests underreporting
- Endoscopy was not mandatory making it difficult to differentiate between stress ulcers and other causes of gastrointestinal bleeding
- Acid suppressant use before ICU admission and enteral nutrition status at baseline were undetermined
- The secondary outcomes should be cautiously interpreted as no P values were provided due to the lack of adjustments for multiple comparisons
- Composite secondary outcome of clinically important events in the ICU may be difficult to interpret as it includes both benefits and risks of the intervention
- Stress ulceration in the ICU is not linked to mortality…maybe morbidity
Discussion:
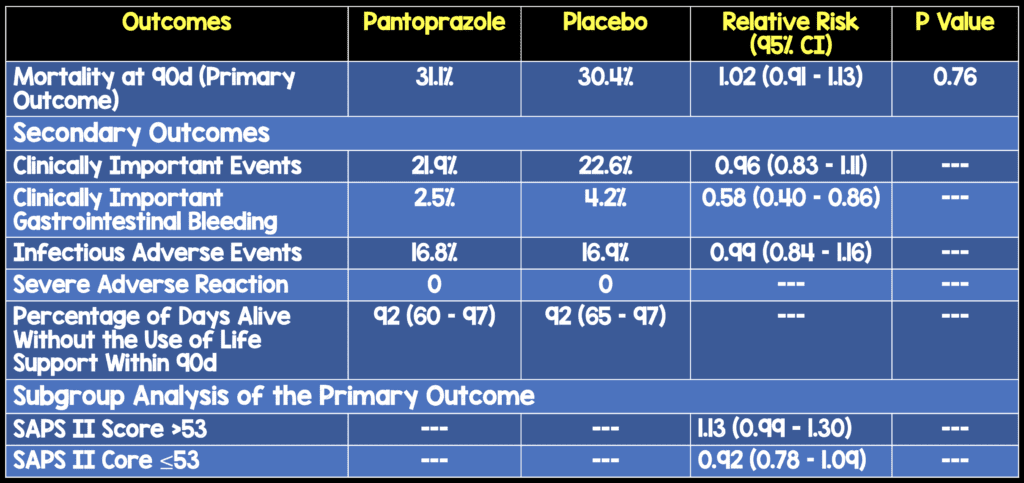
- Similar to previously published studies, the authors found no mortality benefit with routine use of pantoprazole for stress ulcer prophylaxis in critically ill patients5,10
- It is interesting to note that in the sub-group analysis of primary outcome, mortality was higher in the intervention group among patients with a higher SAPS II score on presentation
- Pantoprazole use reduces the risk of clinically important GI bleed when compared to placebo with an absolute risk reduction of 1.7% (NNT=59). This high number underscores the importance of restricting pantoprazole use to highly selected patients with multiple risk factors for GI bleed. A higher number of patients in the placebo group required interventions like endoscopy, coiling or surgery to control the bleed. An outcome that does matter and more reasonable in this study is clinically important GIB…and although a secondary outcome, was reduced with pantoprazole compared to placebo
- The incidence of infectious complications and myocardial ischemia was similar in the two groups
- Though similar number of patients in both groups received enteral nutrition, the infectious complications were not stratified based on enteral nutrition status. Enteral nutrition makes gastric pH more alkaline and some studies suggest increased infectious complications when stress ulcer prophylaxis is combined with enteral feeding11
- No serious adverse reactions were reported with pantoprazole use including anaphylaxis, agranulocytosis, pancytopenia, acute hepatic failure, interstitial nephritis or angioedema
Author’s Conclusion:
Among adult patients in the ICU who were at risk for gastrointestinal bleeding, mortality at 90 days and the number of clinically important events were similar in those assigned to pantoprazole and those assigned to placebo
Clinical Take Home Point:
Though no proven mortality benefit, the reduced incidence of clinically significant GI bleed without increase in infectious and cardiovascular adverse effects suggests a potential benefit of pantoprazole in selected critically ill patients with multiple risk factors for GI bleed
Guest Post By:

Expert Peer Reviewed By:

Jason A. Stamm MD
For More on This Topic Checkout:
- Josh Farkas at PulmCrit: SUP-ICU – Is Pantoprazole the Elixir of Life? Should it Be?
- Adrian Wong at The Bottom Line: SUP-ICU
References:
- Krag M et al. Prevalence and Outcome of Gastrointestinal Bleeding and Use of Acid suppressants in Acutely ill Adult Intensive Care Patients. Intensive Care Med 2015. PMID: 25860444
- Cook D et al. Prophylaxis Against Upper Gastrointestinal Bleeding in Hospitalized Patients. N Engl J Med 2018. PMID: 29949497
- Cook D et al. The Attributable Mortality and Length of Intensive Care Unit Stay of Clinically Important Gastrointestinal Bleeding in Critically ill Patients. Crit Care. 2001. PMID: 11737927
- Krag M et al. Stress Ulcer Prophylaxis in the Intensive Care Unit: An International Survey of 97 Units in 11 Countries. Acta Anaesthesiol Scand 2015. PMID: 25880349
- Alhazzani W et al. Efficacy and Safety of Stress Ulcer Prophylaxis in Critically ill Patients: A Network Meta-Analysis of Randomized Trials. Intensive Care Med 2018. PMID: 29199388
- Alshamsi F et al. Efficacy and Safety of Proton Pump Inhibitors for Stress Ulcer Prophylaxis in Critically ill Patients: A Systematic Review and Meta-Analysis of Randomized Trials. Crit Care 2016. PMID: 27142116
- MacLaren R et al. Histamine-2 Receptor Antagonists vs Proton Pump Inhibitors on Gastrointestinal Tract Hemorrhage and Infectious Complications in the Intensive Care Unit. JAMA Intern Med 2014. PMID: 24535015
- Buendgens L et al. Administration of Proton Pump Inhibitors in Critically ill Medical Patients is Associated with Increased Risk of Developing Clostridium Difficile-Associated Diarrhea. J Crit Care 2014. PMID: 24674763
- Krag M et al. Pantoprazole in Patients at Risk for Gastrointestinal Bleeding in the ICU. N Engl J Med 2018. PMID: 30354950
- Krag M et al. Stress Ulcer Prophylaxis Versus Placebo or No Prophylaxis in Critically ill Patients: A Systematic Review of Randomised Clinical Trials with Meta-Analysis and Trial Sequential Analysis. Intensive Care Med 2014. PMID: 24141808
- Huang H et al. Stress Ulcer Prophylaxis in Intensive Care Unit Patients Receiving Enteral Nutrition: A Systematic Review and Meta-Analysis. Crit Care 2018. PMID: 29374489
Post Peer Reviewed By: Frank Lodeserto, MD (Twitter: @FrankLodeserto) and Salim R. Rezaie, MD (Twitter: @srrezaie)
The post SUP-ICU: Ending the Confusion About Stress Ulcer Prophylaxis in ICU. So I Don’t Give it Right, or do I? appeared first on REBEL EM - Emergency Medicine Blog.