![]()
As a follow-up to last year’s inaugural JGME-ALiEM Hot Topic in Medical Education on the Resident as Teacher role, this week we will be conducting a cross-disciplinary discussion about a unique instructional strategy called team-based learning (TBL). Originally developed by Dr. Larry Michaelson, a professor of Business at the University of Oklahoma, over the past 15-20 years TBL has been increasingly incorporated in health professions education. Prominent in undergraduate medical curricula, TBL focuses on active learning, collaboration, and application to real-world problems. As educators consider its value in postgraduate education, TBL is our “hot topic” for 2016.
Whether you are hearing about TBL for the first time, considering incorporating it into your practice or just curious to stay on top of what’s hot in meded, we invite you to engage in the discussion of the JGME publication entitled “Use of Team-Based Learning Pedagogy for Internal Medicine Ambulatory Resident Teaching” by Balwan et al. using the Twitter hastag #JGMEscholar [free article PDF].
Similar to previous ALiEM-Annals Journal Clubs, a live Google Hangout will be held with the authors and selected experts. Ultimately, a curated summary from discussions (ALiEM blog, Twitter, Google Hangout) will be published back in JGME. Some of your best tweets and blog comments will be featured.
What is Team Based Learning (TBL)?
TBL is an active learning and small group instructional strategy that provides students with opportunities to apply conceptual knowledge through a sequence of activities that includes individual work, teamwork, and immediate feedback. 1 The concept is that sequential activities allow participants to scaffold their learning while tackling problems similar to real practice.
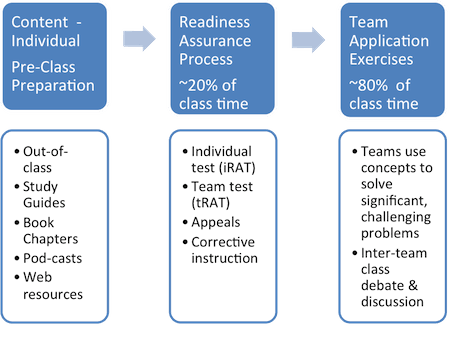
Image from http://www.bradford.ac.uk/educational-development/team-based-learning/TBL-new-diagram.png
1. Advanced, Pre-Class Preparation
The instructor must choose and provide learners with materials (reading assignments, podcasts, videos) that specifically address the learning objectives for the session. Learners are expected to study and review the materials in preparation for the TBL session.
2. Individual Readiness Assurance Test (IRAT)
At the beginning of the instructional session, learners complete a knowledge assessment (typically a multiple choice test) that is directly related to the advance preparatory material. This assessment induces an educational effect, 2 where learners are motivated and accountable for advanced preparation.
3. Team Readiness Assurance Test (TRAT)
After completing the IRAT, the learners split off into their teams and complete the same set of questions previously answered individually in the IRAT. During this exercise the team must develop a consensus about their answers. Ideally there is a mechanism in place that allows team members to know as immediately-as-possible whether or not they have selected the correct answers. This immediate feedback helps them to refine their decision-making processes.
4. Instructor Clarification and Review
Typically this involves a very brief clarification of concepts that a significant number of learners struggled with throughout the readiness assurance tests. Learners must feel confident that they are adequately prepared to use their newly-acquired knowledge during the subsequent the team application exercise.
5. Application Exercise
The application exercise is the most important step: learners are given a problem similar to what they might face in clinical practice. This must be a problem that challenges them and forces them to interpret, calculate, predict, or analyze. At the end of the exercise, all teams must report their responses (near) simultaneously to the group and explain or defend their choice to the group.
What are the perceived benefits of TBL?
- Unlike other small group learning strategies, it allows for large groups of learners to be taught by one content-expert, thus making it scalable. It is appealing to educators who want to promote active and engaged learning without the need for additional instructors.
- It helps to equip learners to function in a team-oriented environment common to Medicine.
- The integrated assessments hold each individual accountable for their preparation and participation. The assessments also allow for early identification of poor performers, while supporting and engaging them through extensive peer teaching.
- A recent BEME review acknowledges the potential of TBL to significantly increase knowledge scores in health professions education. 3 Although the evidence does not clearly demonstrate superiority over other instructional strategies, it is at least as effective.
Featured JGME Paper
Balwan S, Fornari A, DiMarzio P, Verbsky J, Pekmezaris R, Stein J, Chaudhry S. Use of Team-Based Learning Pedagogy for Internal Medicine Ambulatory Resident Teaching. J Grad Med Educ. 2015 Dec;7(4):643-8. doi: 10.4300/JGME-D-14-00790.1. PMID: 26692979. Free PDF
[su_spoiler title=”ABSTRACT” style=”fancy” icon=”caret”]BACKGROUND: Team-based learning (TBL) is used in undergraduate medical education to facilitate higher-order content learning, promote learner engagement and collaboration, and foster positive learner attitudes. There is a paucity of data on the use of TBL in graduate medical education. Our aim was to assess resident engagement, learning, and faculty/resident satisfaction with TBL in internal medicine residency ambulatory education.
METHODS: Survey and nominal group technique methodologies were used to assess learner engagement and faculty/resident satisfaction. We assessed medical learning using individual (IRAT) and group (GRAT) readiness assurance tests.
RESULTS: Residents (N = 111) involved in TBL sessions reported contributing to group discussions and actively discussing the subject material with other residents. Faculty echoed similar responses, and residents and faculty reported a preference for future teaching sessions to be offered using the TBL pedagogy. The average GRAT score was significantly higher than the average IRAT score by 22%. Feedback from our nominal group technique rank ordered the following TBL strengths by both residents and faculty: (1) interactive format, (2) content of sessions, and (3) competitive nature of sessions.
CONCLUSIONS: We successfully implemented TBL pedagogy in the internal medicine ambulatory residency curriculum, with learning focused on the care of patients in the ambulatory setting. TBL resulted in active resident engagement, facilitated group learning, and increased satisfaction by residents and faculty. To our knowledge this is the first study that implemented a TBL program in an internal medicine residency curriculum.[/su_spoiler]
Google Hangout with Drs. Balwan, Jalali, and Sherbino (Thu, Jan 14 at 12:00 EST)
Hot Topics Questions
Remember to respond using #JGMEscholar hashtag if joining the discussion via Twitter.
- If knowledge is socially constructed (i.e. how an individual organizes, perceives and attends to information is influenced by the interaction of other individuals in their environment) then the idiosyncrasies of the make-up of a particular team may lead to different learning outcomes between teams. Should the organization of a team be random or specifically cultivated?
- The TBL evaluation data presented conflicting results. The engagement survey, which used individual responses, indicated that 93% of residents and 88% of faculty agreed or strongly agreed that “I/residents contributed my/their fair share to session discussions.” Yet, the nominal group technique, which used a quasi-consensus process, noted an imbalance of resident participation from both faculty and resident evaluation groups. How do you explain this inconsistency?
- While the study did not compare the required resources or time necessary to run a TBL session, the discussion implied that this instructional method was more resource intensive for faculty. How can we motivate faculty to invest in learning methods that require more work than their current practice?
- How does the team-based decision-making process improve a learner’s independent decision-making typically required of clinical practice?
Disclaimer: We reserve the right to use any and all tweets to #JGMEscholar and comments below in a commentary piece for a Journal of Graduate Medical Education publication as a curated conclusion piece for this hot topic discussion. Your comments will be attributed. We thank you in advance for your contributions.
Author information

The post Team-Based Learning: 2016 JGME-ALiEM Hot Topics in Medical Education appeared first on ALiEM.