
 The DINAMO Study: Efficacy and Safety of Non-Antibiotic Outpatient Treatment in Mild Acute Diverticulitis
The DINAMO Study: Efficacy and Safety of Non-Antibiotic Outpatient Treatment in Mild Acute Diverticulitis
James C. Fletcher, MD, FACEP and Nicholas Slattery, MD
Background: Diverticulitis is a common finding amongst Emergency Department patients, accounting for more than 360,000 visits in 2013 alone1. Additionally, the rate of diverticulitis appears to be increasing among both patients presenting to the Emergency Department and the population in general. Despite its frequency, the majority of cases of acute diverticulitis are uncomplicated, and can be effectively managed on an outpatient basis2. Antibiotic therapy has long been a mainstay of treatment, as the primary etiology of acute diverticulitis and colitis has historically been assumed to be infectious in nature. The scientific basis for antibiotic treatment is rather weak, however, and is largely based on decades-old data demonstrating a reduction in the incidence of both severe complications and the need for surgical intervention. Additionally, several recent clinical trials have offered a challenge to the long-held dogmatic belief of antibiotic necessity3,4. Despite these results, however, a lack of prospective5 data specifically addressing the question of non-antibiotic therapy in the outpatient population makes the applicability of such an approach to Emergency Department patients unclear. As such, the DINAMO study is of particular interest to emergency physicians seeking to determine the most appropriate treatment regimen for a condition that they encounter frequently.
The Paper: Mora-López, L. et al. Efficacy and Safety of Nonantibiotic Outpatient Treatment in Mild Acute Diverticulitis (DINAMO Study). Annals of Surgery, 2021. PMID: 34183510 [Access on Read by QxMD]
Clinical Question: Is it necessary to prescribe antibiotics to all patients undergoing outpatient management for mild diverticulitis as identified on CT scan?
What They Did:
- Multicenter, open label, non-inferiority randomized control trial
- Conducted at 15 colorectal surgery units at acute care secondary and tertiary hospitals in Catalonia, Spain from November 2016 – January 2020
- Patients Randomized To:
- Control Group: Outpatient therapy with antibiotics + pain medications and anti-inflammatories
- Experimental Group: Pain meds/anti-inflammatories alone
- Non–inferiority margin set at 7% based on previous outpatient studies of acute diverticulitis
Outcomes:
- Primary Outcome: Hospital admission
-
Secondary Outcome(s):
- Repeat visits to Emergency Department
- Need for emergency surgery
- Pain control at various time points
Inclusion Criteria:
- Age 18-80 years
- Acute Diverticulitis identified on CT scan
- Modified Neff Classification score of 0
- No episodes of acute diverticulitis in last 3 months
- No antibiotics (for any reason) in the 2 weeks prior to presentation
- No significant comorbidities**
- Good symptom control in the ED
- Immunocompetence
- Ability to provide written informed consent
- Adequate cognitive capacity (defined as “the ability to read and understand the description of the study and to provide signed informed consent”)
- Adequate family support (the patient had someone able to take care of him/her and provide help as necessary.)
- A maximum of ONE of the following:
- T > 38C or < 36C
- WBC > 12,000/mL or < 4,000/mL
- HR > 90 bpm
- RR >20 rpm
- C-reactive Protein >15 mg/dL.
Exclusion Criteria:
- Women who were pregnant or breastfeeding
- Age <18 or >80 years
- Allergy to any of the study drugs
- Acute diverticulitis with a Modified NEFF classification of Stage 1 or higher
- History of inflammatory bowel disease
- Presence of significant comorbidities**
- Immunosuppression or immunocompromise
- Poor symptom control at the ED (VAS ≥5)
- Presence of systemic inflammatory response syndrome (SIRS) or sepsis
**“Significant comorbidities” include: diabetes mellitus with organ involvement (retinopathy, angiopathy, nephropathy), emergency assistance for a cardiogenic event in the last 3 months (acute myocardial infarction, angina, heart failure), decompensation of chronic liver disease in the last 3 months, end-stage renal disease, active neoplastic disease, any history of hematologic malignancy, active human immunodeficiency virus infection with low CD4 count (AIDS), long term corticosteroid treatment, ongoing immunosuppressant therapy, history of solid-organ transplant, prior splenectomy, any genetic immunodeficiency.
Study Protocol:
- Patients were chosen and enrolled from those presenting to the Emergency Department
- Medical treatment was initiated in the ED, with patients receiving IV medications for symptom control initially.
- Once appropriate symptom control was achieved, patients were discharged home with medical treatment and diet recommendations.
- Experimental Group: Ibuprofen 600 mg PO Q8H alternating with Acetaminophen 1g PO Q8H
- Control Group: Same as above plus Amoxicillin/Clavulanic acid 875/125 PO Q8H
- Therapy was continued for seven days in both groups
- If good symptomatic control was not achieved after a maximum of 24 hours of observation in the ED, patients were admitted for IV treatment, and therefore did not enter the study.
- Enrolled patients received follow-up assessments at 2, 7, 30, and 90 days after their initial presentation. These follow-up visits were conducted by staff surgeons of the respective colorectal surgery units.
- Follow-up assessments included physical examination, evaluation of the clinical evolution of patient’s symptoms, and assessment of adherence to the treatment regimen.
- The degree of pain experienced by the patients was recorded at each assessment on a visual analogue scale (VAS, 0 – 10).
- If clinical worsening or poor symptomatic control was detected at any time, the patient was referred to the Emergency Department. Patients also received counseling regarding symptoms that should prompt a return to emergency care and were encouraged to consult the ED at their own discretion if these occurred.
Results:
- A total of 480 patients were enrolled
- 242 were randomized to the non-antibiotic group
- 238 were randomized into the group receiving antibiotic therapy
- There was NO STATISTICALLY SIGNIFICANT difference in hospitalizations. 14/238 patients in the antibiotic group required hospitalization, compared to 8/242 in the non-antibiotic group (2.58% difference, 95% CI 6.32 to 1.17)
- There was NO STATISTICALLY SIGNIFICANT difference in return visits to the Emergency Department. 16/238 patients in the antibiotic group had a repeat visit to the ED compared to 17/242 in non-antibiotic group (-0.3% difference, 95% CI 4.22 to 4.83)
- Among those patients who did return to the Emergency Department, the antibiotic group had a longer median time from initial presentation until repeat ED visit (17 days vs. 13 days)
- Interestingly, pain control was numerically better at 2-day follow-up among the non-antibiotic group. 13/230 patients in antibiotic group were found to have poor pain control as compared to 5/221 in the non-antibiotic group. This difference was not deemed to be statistically significant, however. (3.39% difference, 95% CI 6.96 to -0.18)
- There was no significant difference in pain control between the two groups at any of the other follow-up intervals.
- NO PATIENT in either group required emergency surgery during the study period
Strengths:
- Randomized, controlled, multi-center study that is statistically well-powered – target enrollment of 230 patients per arm was achieved.
- This study examined and enrolled patients who initially presented to the Emergency Department, and treatment was initiated in the ED.
- This study builds on data from previous studies in determining if a therapeutic approach is more broadly applicable
- A well-defined, and standardized radiographic scoring system was used to identify appropriate patients
- The study’s inclusion criteria limited the enrollment of patients who were at higher risk for complications from diverticulitis.
- The experimental and control groups were well-matched with regard to baseline demographics
- The secondary outcome of pain control was measured using a previously validated scale/system
- Loss to follow-up was less than anticipated
- Loss rate of 10% at 90 days was factored into the study’s initial power calculations.
- The study addresses a clinically valid question and examined patient-centered outcomes (need for emergency surgery, pain control, frequency of return visits to the ED)
Weaknesses:
- Strict inclusion criteria may limit generalizability
- This is a non-blinded study. Although no significant difference was reported in terms of hospitalization, return visits to the ED, pain control, or recovery, the non-blinded nature of the study does introduce the potential for selection, confirmation, and/or reporting bias.
- There is no mention of what interventions were used to achieve control of symptoms prior to enrollment and randomization. Additionally, study protocols do not account for additional medications needed/utilized for appropriate symptom control as an outpatient (such as anti-emetics, stool softeners, etc.)
- Study patients were initially managed in the Emergency Department for up to 24 hours – far longer than would be the norm in most EDs in the United States.
- The use of a radiographic scoring system to determine disease severity may not appropriately correlate with symptom severity nor likelihood of acute complication.
Discussion:
This well-powered, prospective, randomized control trial examined a cohort of patients presenting to the Emergency Department who were found to have mild, uncomplicated acute diverticulitis on CT scan. Study protocols were based on the results of previous studies, as well as current clinical guidelines. Patients were enrolled in real time by clinicians caring for them in the ED, and both the study inclusion criteria and clinical judgement of the enrolling providers assured that the patients selected were deemed appropriate for outpatient management. After being selected and screened to assure they met inclusion criteria, patients were then randomized to receive either “standard” outpatient therapy of pain medications plus antibiotics, or a course of pain medications alone. Adequacy of symptom control was assured prior to enrollment, so patients’ decisions regarding enrollment were not surreptitiously motivated by a desire to gain what they might see as a more favorable treatment. The severity of their symptoms was assessed in follow-up by colorectal surgery specialists, and the patients’ overall recovery (defined as return to normal diet, absence of symptoms, and return to normal activities) was tracked at each follow-up visit. Study participants were referred back to the Emergency Department in the event of clinical deterioration, and each patient received clear and careful instructions as to symptoms/issues that should prompt a return to emergency care. These combined protocols created an effective “fail-safe” mechanism, minimizing the risk of potential harm to the enrolled patients. Ultimately, no significant differences were found in outcomes amongst the two groups, including the need for hospitalization, the occurrence of severe complications, and recovery time.
By far, the most commonly levied criticism of this study – and perhaps its greatest weakness – lies in its extremely strict inclusion criteria. Although the full impact is uncertain, this study’s exclusion of a significant number of patients seems likely to both introduce selection bias and to limit its generalizability. While the published baseline demographic data were similar for both study groups, it is worth noting that as a whole this study looked at younger (average age = 57 for antibiotic group, 59 for non-antibiotic group), otherwise healthy persons suffering from mild cases of acute diverticulitis. Despite the potential impact on its generalizability, however, It is unclear as to whether or not the study’s limited inclusion criteria actually impacts the applicability of its conclusions – as older, sicker, and/or more complicated patients would seem unlikely to be deemed appropriate for outpatient management and discharge from the Emergency Department.
The importance of close follow-up was highlighted within the study design, as patient follow-up assessments were an integral part of both data gathering and ongoing clinical management. However, two environmental factors would seem to limit the generalizability of the follow-up regimen – specifically, the study’s execution at specialized colorectal surgery centers, and its completion in a European nation with a centralized National Health System. For many physicians practicing in the Emergency Department setting, facilitation of such close specialist follow-up may not be possible. Given the potential difficulties encountered by emergency clinicians in arranging appropriate follow-up care, consideration of a “wait-and-see” approach – wherein patients are discharged home with an antibiotic prescription, but instructed not to begin them unless symptoms fail to improve after a period of time – might be pertinent. Although the DINAMO study itself did not specifically address this possibility, the “wait-and-see” approach is commonly utilized in the outpatient management of other minor infectious processes (sinusitis, acute otitis media, etc.), and logical extrapolation of the study’s results would seem to indicate that it could be safely applied to the outpatient treatment of acute diverticulitis without an increase in patient risk. Nevertheless, the fact that the DINAMO study protocols were tooled to include follow-up assessments as well as strict “return to care” instructions highlights the importance of both in the appropriate outpatient management of mild diverticulitis.
Despite its limitations, this paper adds to the growing body of information challenging the dogmatic “necessity” of antibiotic therapy in the treatment of mild acute diverticulitis. Notably, this study’s findings are in line with the American Gastroenterological Association’s 2021 Clinical Practice Updates, which encourage antibiotic use “selectively rather than routinely” in cases of mild diverticulitis6. Although it is unlikely that the overall community standard of practice will change until additional consensus guidelines and medical references align with a non-antibiotic approach, the results of the DINAMO study offer evidence to the Emergency Physician that an “antibiotics for all” approach in managing acute diverticulitis – especially in patients who are appropriate for outpatient management – is neither pertinent nor necessary.
Author Conclusion: “Nonantibiotic outpatient treatment of mild AD is safe and effective and is not inferior to current standard treatment.”
Clinical Bottom Line: Otherwise healthy patients presenting to the Emergency Department with mild acute diverticulitis, no signs of severe infection/sepsis, and who achieve good symptom control in the ED may be discharged home with symptomatic management and close follow-up only, and may not require antibiotic therapy.
Guest Post By:

James C. Fletcher, MD, FACEP, FAAEM
Clinical Assistant Professor
Department of Emergency Medicine
Brody School of Medicine at East Carolina University
Twitter: @jfletchermd
![]()
Nicholas Slattery, MD
Emergency Medicine Resident
ECU Health Medical Center
Brody School of Medicine at East Carolina University
References:
- Bollom A et al. Emergency Department Burden of Diverticulitis in the USA, 2006-2013. Dig Dis Sci. 2017. PMID: 28332105
- Biondo S et al. Outpatient versus hospitalization management for uncomplicated diverticulitis: a prospective, multicenter randomized clinical trial (DIVER Trial). Ann Surg. 2014. PMID: 23732265
- Daniels L et al. Randomized clinical trial of observational versus antibiotic treatment for a first episode of CT-proven uncomplicated acute diverticulitis. Br J Surg. 2017. PMID: 27686365
- Chabok A et al. AVOD Study Group. Randomized clinical trial of antibiotics in acute uncomplicated diverticulitis. Br J Surg. 2012. PMID: 22290281
- Estrada Ferrer O et al. Selective non-antibiotic treatment in sigmoid diverticulitis: is it time to change the traditional approach? Tech Coloproctol 2016. PMID: 27053254
- Peery AF et al. AGA Clinical Practice Update on Medical Management of Colonic Diverticulitis: Expert Review. Gastroenterology 2021. PMID: 33279517
Additional FOAMed Resources:
- European Society of Coloproctology: Paper of the Month – December 2021
- Gastroenterology Advisor: Nonantibiotic Outpatient Therapy Safe and Effective for Mild Acute Diverticulitis
- NEJM Journal Watch Summary: Are Antibiotics Required for Mild Acute Diverticulitis?
SUPPLEMENT 1: Modified Neff criteria for classification of acute diverticulitis.
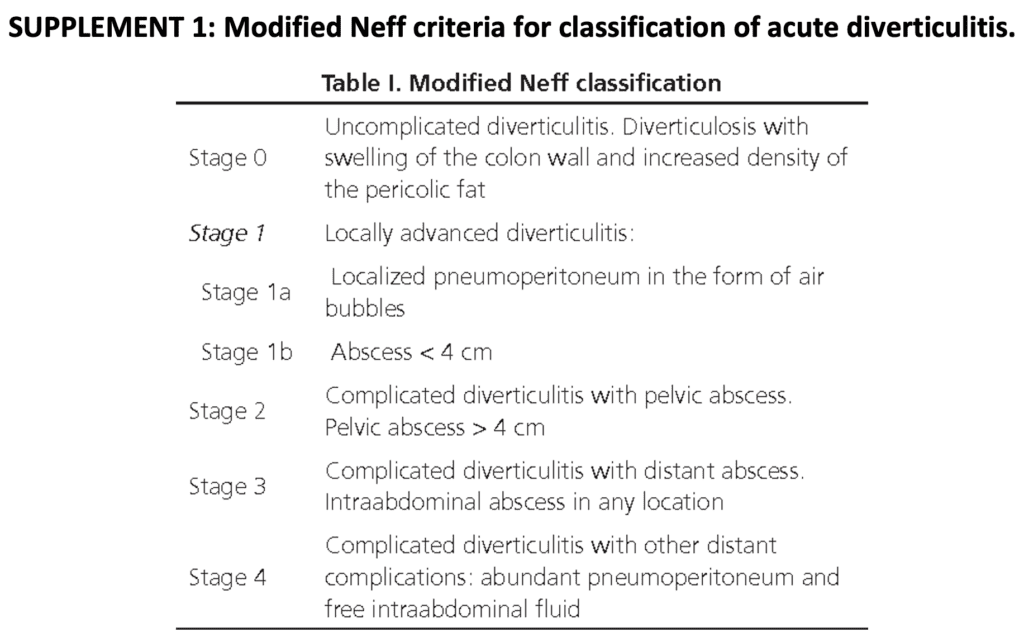
From: Mora López et al. Rev Esp Enferm Dig. 2017. PMID: 28376628
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post The DINAMO Study: Efficacy and Safety of Non-Antibiotic Outpatient Treatment in Mild Acute Diverticulitis appeared first on REBEL EM - Emergency Medicine Blog.