
 There are more than 750,000 cases of severe sepsis and septic shock in the US each year. Most patients who present with sepsis receive their initial care in the emergency department. In 2001, there was a landmark study by Rivers et al [1] that reported that among patients with severe sepsis or septic shock mortality was significantly lower among those who received a 6 hour protocol of Early Goal-Directed Therapy (EGDT) (i.e. 30.5% vs 46.5%). The premise of EGDT was that “usual care” lacked aggressive, timely assessment and treatment. The EGDT protocol used central venous catheterization (CVC) to monitor central venous pressure (CVP) and central venous oxygen saturation (SCVO2) to guide the use of intravenous fluids (IVFs), vasopressors, packed red blood cell (PRBC) transfusions, and dobutamine in order to achieve pre-specified physiological targets. Since the publication of this landmark article, physicians have become more aggressive in the management of sepsis which raises the question of whether all elements of the protocol are still necessary.
There are more than 750,000 cases of severe sepsis and septic shock in the US each year. Most patients who present with sepsis receive their initial care in the emergency department. In 2001, there was a landmark study by Rivers et al [1] that reported that among patients with severe sepsis or septic shock mortality was significantly lower among those who received a 6 hour protocol of Early Goal-Directed Therapy (EGDT) (i.e. 30.5% vs 46.5%). The premise of EGDT was that “usual care” lacked aggressive, timely assessment and treatment. The EGDT protocol used central venous catheterization (CVC) to monitor central venous pressure (CVP) and central venous oxygen saturation (SCVO2) to guide the use of intravenous fluids (IVFs), vasopressors, packed red blood cell (PRBC) transfusions, and dobutamine in order to achieve pre-specified physiological targets. Since the publication of this landmark article, physicians have become more aggressive in the management of sepsis which raises the question of whether all elements of the protocol are still necessary.
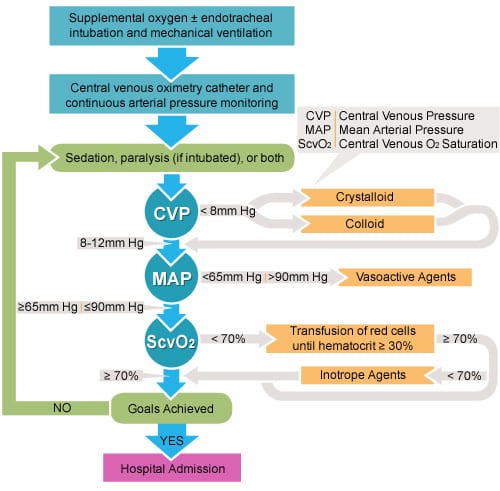
What was the 6 Hour EGDT Protocol from the 2001 Rivers Study?
What are the newest studies evaluating sepsis management?
- Protocolized Care for Early Septic Shock The ProCESS Trial [2]
- Australasian Resuscitation in Sepsis Evaluation The ARISE Trial [3]
The ProCESS Trial
What they did:
- Multicenter, Randomized Control Trial of 1341 patients with septic shock (31 EDs in the US) randomized to one of 3 arms:
- Protocol Based EGDT
- Protocol-Based Standard Therapy without use of CVC, administration of inotropes, or blood transfusions
- Usual Care
Primary Endpoint: 60 day in-hospital mortality
Results:
- 92 deaths in EGDT group (21.0%)
- 81 deaths in Protocol Based Standard Therapy (18.2%)
- 86 deaths in Usual Care (18.9%)
- No statistical difference in 90 day and 1 year mortality
Limitations:
- Cannot be sure that all elements critical to the success of the Rivers et al. protocol were adhered to 100% of the time in the EGDT arm
- Only patients who were recognized early as septic shock were enrolled in this study (i.e. Early IVF with refractory hypotension and early antibiotics then randomized into one of three arms), not delayed presentations of septic shock
- This study was performed in large tertiary care centers in the US, so it is not clear how this study would translate into other settings (i.e. Smaller, rural, community EDs)
Study Conclusion: Protocol-based resuscitation of patients with septic shock does not improve 60 day mortality

The ARISE Trial
What they did:
- Prospective, Multicenter, Randomized Control Trial of 1600 patients presenting to an ED with early septic shock
- 51 Centers (45 EDs in Australia and/or New Zealand and 6 EDs in Finland, Hong Kong, and Ireland)
- Patients randomized to EGDT vs Usual care
Outcomes:
- All Cause 90 Day Mortality
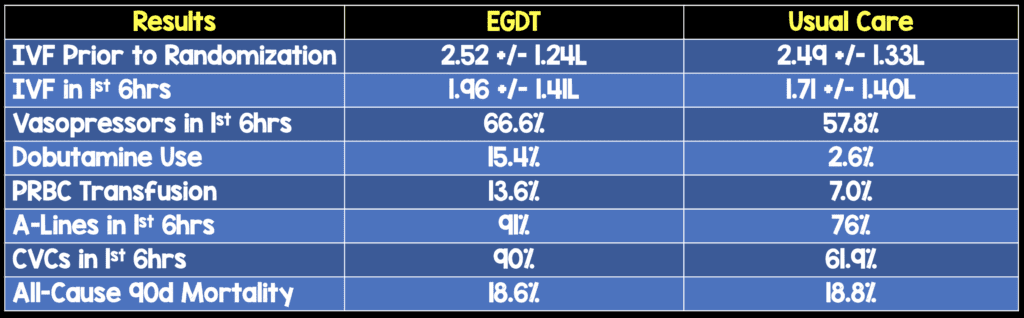
Results:
Limitations:
- Low APACHE scores (15.4 in EGDT vs 15.8 in Usual Care) compared to the ProCESS Trial (20.8 in EGDT, 20.6 in Protocol Based Care, and 20.7 in Usual Care) but most patients had lactate levels ≥4 in both groups (46.0% in EGDT vs 46.5% in Usual Care) which means this was still a sick patient population
Study Conclusion: In patients presenting to the Emergency Department with Early Septic Shock, EGDT did not reduce all-cause mortality at 90 days
My Thoughts on These Studies:
The ProCESS Trial:
- If patients in septic shock are identified early, given IVF early, and antibiotics early, then the CVC and central readings should not matter in the care of septic shock patients
- This study did not create a clear, superior method in management of septic shock patients, but did make it clear that no one resuscitative pathway is bad or better. This gives various sites flexibility in management after early recognition, early IVFs, and early antibiotics.
- The cohort of patients in this study is different than the cohort of patients in the 2001 Rivers et al study. Although Vital Signs and APACHE scores were similar between the two studies, the mortality rates were significantly different (i.e. EGDT mortality decreased from 47 –> 31% [NNT = 6] in the 2001 Rivers et al study and in the ProCESS trial mortality rates were 21% in EGDT, 18.2% in protocolized care, and 18.9% in usual care arms)
- The 2001 Rivers et al study has changed how we manage sepsis (i.e. We are more aggressive in identifying these patients, and our “usual care” has changed to early identification, early IVFs and early antibiotics), which may explain why we have lower mortality rates now compared to the 2001 Rivers et al study
The ARISE Trial
- This trial took place in tertiary and non-tertiary metropolitan and rural EDs, which allows for more generalizability of results
- This trial was not a blinded study, due to the requirements of EGDT. The authors stated that they tried to minimize bias through “central randomization, concealment of study-group assignments before randomization to avoid selection bias and the use of a robust primary outcome that would not be subject to observer bias.“
- Again the mortality rate of this study was lower than the 2001 Rivers et al study (i.e. EGDT mortality decreased from 47 –> 31% [NNT = 6] in the 2001 Rivers et al study and in the ARISE trial mortality rates were 18.6% in EGDT and 18.8% in usual care arms)

Clinical Take Home Message:
Simply put, in septic shock, we need to be AGGRESSIVE in our care EARLY. If patients are identified EARLY, given IVF EARLY, and antibiotics EARLY, again the key being EARLY, then the pathway used afterwards (i.e EGDT, Protocolized, or “usual care”) is less important in management and resuscitation.
References:
- Rivers E et al. Early Goal-Directed Therapy in the Treatment of Severe Sepsis and Septic Shock. NEJM 2001. PMID: 11794169
- ProCESS Investigators. A Randomized Trial of Protocol-Based Care for Early Septic Shock. NEJM 2014. PMID: 24635773
- ARISE Investigators. Goal-Directed Resuscitation for Patients with Early Septic Shock. NEJM 2014. PMID: 25272316
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)
For More About the Above Studies Checkout:
The ProCESS Trial
- Scott Weingart at EMCrit: Podcast 120 – The ProCESS Trial with Derek Angus
- Seth Trueger at MDAware: Trust the ProCESS
- Michelle Lin at ALiEM: ProCESS Study – Identify Sepsis Early and Treat Aggressively
- Ken Milne at The SGEM: SGEM#69 – Cry Me a River (Early Goal Directed Therapy) ProCESS Trial
- Simon Carley at St. Emlyn’s: JC – Is Early Goal Directed Therapy Dead?
The ARISE Trial
- Scott Weingart at EMCrit: Podcast 134 – ARISE has Arisen
- Ryan Radecki at EMLit of Note: ARISE, and Cast Off the Shackles of EGDT
- Oliver Flower at Intensive Care Network: The Arise Trial – Arisen
- Steve Mathieu at The Bottom Line: ARISE – Australian Resuscitation In Sepsis Evaluation Randomised Control Trial
The post The New Age of Sepsis Management appeared first on REBEL EM - Emergency Medicine Blog.