
 Background: Transfusion thresholds for anemia have large variations in clinical practice. This is especially true in patients with acute myocardial infarction (AMI). Part of the reason for this is the lack of high-quality data. There was a large, randomized trial looking at restrictive vs liberal transfusion strategies in non-crashing GI bleeding [2] which found a restrictive transfusion strategy was superior, however patients with AMI were excluded.
Background: Transfusion thresholds for anemia have large variations in clinical practice. This is especially true in patients with acute myocardial infarction (AMI). Part of the reason for this is the lack of high-quality data. There was a large, randomized trial looking at restrictive vs liberal transfusion strategies in non-crashing GI bleeding [2] which found a restrictive transfusion strategy was superior, however patients with AMI were excluded.
Paper: Ducrocq G et al. Effect of a Restrictive vs Liberal Blood Transfusion Strategy on Major Cardiovascular Events Among Patients With Acute Myocardial Infarction and Anemia: The REALITY Randomized Clinical Trial. JAMA 2021. PMID: 33560322 [Access on Read by QxMD]
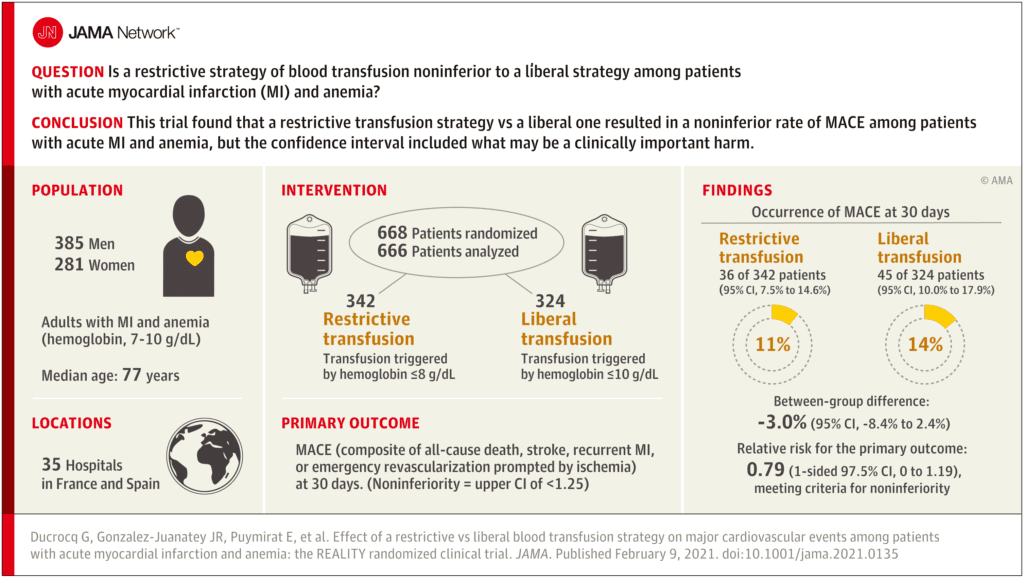
Clinical Question: Is a restrictive strategy of blood transfusion noninferior to a liberal strategy among patients with acute myocardial infarction and anemia?
What They Did:
- Restrictive and Liberal Transfusion Strategies in Patients With Acute Myocardial Infarction (REALITY)
- Open label, noninferiority, randomized controlled trial performed in 35 hospitals in France and Spain
- Patients randomized to:
- Restrictive transfusion: Transfusion triggered by hemoglobin ≤8g/dL
- Liberal transfusion: Transfusion triggered by hemoglobin ≤10g/dL
Outcomes:
-
Primary: Major adverse cardiovascular events (MACE) at 30d
- Composite of all-cause death, stroke, recurrent MI, or emergency revascularization prompted by ischemia
- Noninferiority required the upper bound of the 1-sided 97.5% CI be <1.25
-
Secondary:
- Individual components of the primary outcome at 30d
Inclusion:
- ≥18 years of age
- Have AMI (with or without STEMI + a combination of ischemic symptoms occurring in the 48hrs before admission + elevation of biomarkers of myocardial injury)
- Hemoglobin level between 7 and 10g/dL
Exclusion:
- Shock at the time of randomization (SBP <90mmHg with clinical signs of low output or requiring inotropic drugs)
- MI occurring after percutaneous coronary intervention or coronary artery bypass grafting
- Life-threatening or massive ongoing bleeding (judged by the investigator)
- Blood transfusion in the past 30d
- Malignant hematologic disease
Results:
- 668 patients randomized
- 666 completed 30d follow-up
- Restrictive transfusion protocol: 35.7% received transfusion (342 total units of PRBCs)
- Liberal transfusion protocol: 99.7% received transfusion (758 total units of PRBCs)
-
MACE at 30d (Primary Outcome):
- Restrictive Transfusion Protocol: 11%
- Liberal Transfusion Protocol: 14%
- Difference -3.0%; 95% CI -8.4% to 2.4%
- RR 0.79; 1-sided 97.5% CI; 0.00 – 1.19 Meets non-inferiority threshold
- All-Cause Death at 30d:
- Restrictive Transfusion Protocol: 5.6%
- Liberal Transfusion Protocol: 7.7%
- Recurrent MI at 30d:
- Restrictive Transfusion Protocol: 2.1%
- Liberal Transfusion Protocol: 3.1%
- Emergency Revascularization Prompted by Ischemia at 30d:
- Restrictive Transfusion Protocol: 1.5%
- Liberal Transfusion Protocol: 1.9%
- Nonfatal Ischemic Stroke at 30d:
- Restrictive Transfusion Protocol: 0.6%
- Liberal Transfusion Protocol: 0.6%
Strengths:
- Asks a clinically important question
- Patients were consecutively enrolled into the trial
- Baseline characteristics of patients were balanced between groups
- Follow up data was complete for all 666 patients who were randomized
Limitations:
- Small size did not allow for powering to evaluate superiority of either strategy
- Primary outcome is a composite endpoint where all of the outcomes are not clinically equivalent.
- Open-label trial (i.e. unblinded) which may introduce bias, but it is unclear how that bias would affect the results
- Patients could qualify for transfusion at any time during hospitalization. In other words, some patients may have been enrolled after heart catheterization
- Only looked at 30d outcomes and therefore long-term effects of transfusion strategies is unknown
Discussion:
- There was statistical noninferiority of the restrictive transfusion strategy vs the liberal transfusion strategy. This was seen in the per protocol and intention to treat populations as well adding some validity to this outcome. However, the 97.5% CI ranges could include a clinically important harm.
- A 25% relative increase as the margin for noninferiority, which is what was used in this trial, is fairly conservative
- Another way to say this is that the observed confidence interval limit ranges up to an 18% increase in cardiac events would be clinically meaningful
- Despite having a composite primary outcome of unequal clinical endpoints, interestingly the difference in the primary outcome in this study was not driven by the subjective, less important component (i.e. revascularization), but rather a difference in the more objective outcome (i.e. mortality) and to a lesser extent MI
- A restrictive transfusion protocol in the setting of AMI has some potential benefits compared to a liberal strategy:
- Reduced use of scarce blood resources
- 0 Units Transfused: Restrictive 220 vs Liberal 1
- 1 Unit Transfused: Restrictive 25 vs Liberal 43
- 2 Units Transfused: Restrictive 62 vs Liberal 128
- 3 Units Transfused: Restrictive 19 vs Liberal 54
- ≥4 Units Transfused: Restrictive 19 vs Liberal 54
- Reduced adverse effects from transfusion
- Cost savings
- Reduced use of scarce blood resources
- Currently the MINT trial is underway [Link is HERE] which is randomized clinical trial of 3500 patients and will hopefully shed some more light on which transfusion strategy is better
Author Conclusion: “Among patients with acute myocardial infarction and anemia, a restrictive compared with a liberal transfusion strategy resulted in a noninferior rate of MACE after 30 days. However, the CI included what may be a clinically important harm.”
Clinical Take Home Point: Unfortunately, this trial does not answer the question of a restrictive vs liberal transfusion strategy in patients with anemia and AMI. It appears the theoretical benefits of a restrictive transfusion strategy make pragmatic sense, however there could still be some potential harms using this strategy. Which strategy is used will most likely be dependent on clinician judgment and we will just have to wait for further trials to clarify this question.
References:
- Ducrocq G et al. Effect of a Restrictive vs Liberal Blood Transfusion Strategy on Major Cardiovascular Events Among Patients With Acute Myocardial Infarction and Anemia: The REALITY Randomized Clinical Trial. JAMA 2021. PMID: 33560322
- Villanueva C et al. Transfusion Strategies for Acute Upper Gastrointestinal Bleeding. NEJM 2013. PMID: 23281973
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)
The post The REALITY Trial: Restrictive vs Liberal Blood Transfusion in Patients with AMI and Anemia appeared first on REBEL EM - Emergency Medicine Blog.