
 Background: Multiple guidelines recommend tramadol or NSAIDs as 1stline treatment for patients with osteoarthritis (OA). Tramadol is viewed as a weak opioid because it binds to the mu receptor at a significantly lower affinity than morphine.It also inhibits the reuptake of serotonin and norepinephrine. Tramadol is converted in the liver via CYP2D6 which can cause some issues. The big issue is that CYP2D6 activity varies among patients and this is important because you don’t know how much opiate the patient is actually receiving (i.e. the same dose of tramadol will have widely different effects from patient to patient). Not only is tramadol potentially not giving pain relief, but patients often return to the ED for common side effects of tramadol including nausea/vomiting, dizziness, constipation, etc. Because of it’s multiple mechanisms of action, potential drug-drug interactions, and lowering of the seizure threshold, the safety of tramadol has been brought to question.
Background: Multiple guidelines recommend tramadol or NSAIDs as 1stline treatment for patients with osteoarthritis (OA). Tramadol is viewed as a weak opioid because it binds to the mu receptor at a significantly lower affinity than morphine.It also inhibits the reuptake of serotonin and norepinephrine. Tramadol is converted in the liver via CYP2D6 which can cause some issues. The big issue is that CYP2D6 activity varies among patients and this is important because you don’t know how much opiate the patient is actually receiving (i.e. the same dose of tramadol will have widely different effects from patient to patient). Not only is tramadol potentially not giving pain relief, but patients often return to the ED for common side effects of tramadol including nausea/vomiting, dizziness, constipation, etc. Because of it’s multiple mechanisms of action, potential drug-drug interactions, and lowering of the seizure threshold, the safety of tramadol has been brought to question.
What They Did:
- Five, sequential, propensity score-matched cohort study
- Used The Health Improvement Network (THIN) electronic medical record database derived from records of general practitioners in the UK
- Examine the association of tramadol with all-cause mortality among patients with OA and one-year outcomes
Outcomes:
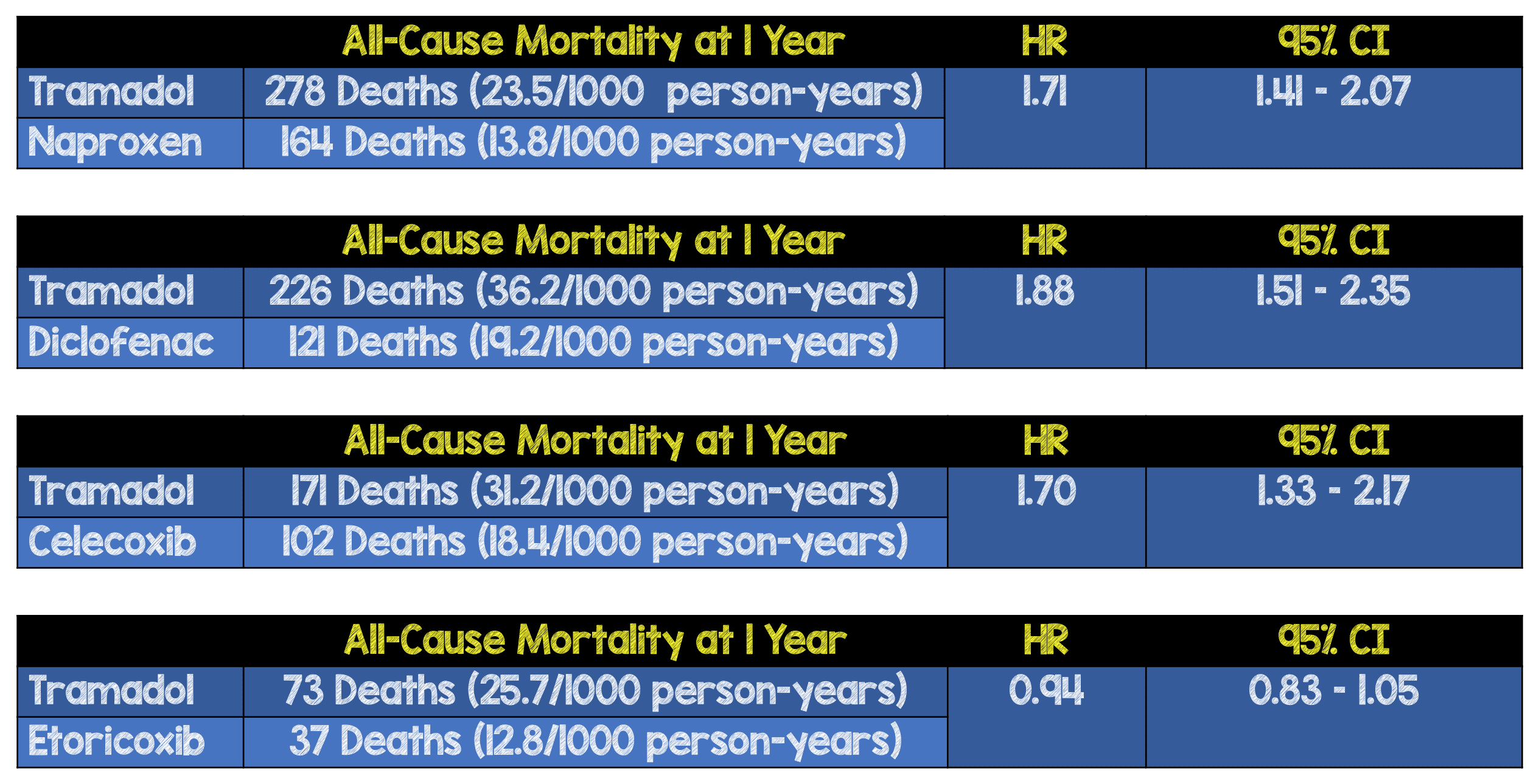
- Primary: All-cause mortality within 1 year after initial tramadol prescription, vs 5 other pain relief medications:
- Naproxen
- Diclofenac
- Celcoxib
- Etoricoxib
- Codeine
Inclusion:
- Age >50 years
- Knee, hip, or hand OA
- Visiting participating GP offices
- 1 year of continuous medication prior to study
Exclusion:
- Cancer
- Opioid use disorder
- Missing values for BMI, drinking habits, smoking status, or Townsend Deprivation Index
Results:
- Initial Prescriptions:
- Tramadol (n = 44,451 pts)
- Naproxen (n = 12, 397 pts)
- Diclofenac (n = 6,512 pts)
- Celcoxib (n = 5,674 pts)
- Etoricoxib (n = 2,964 pts)
- Codeine (n = 16,922 pts)
- 88,902 patients included in the analysis
- Mean age 70.1 years
- Tramadol prescriptions increased from 3.4% in 2000 to 11.1% in 2013
- Naproxen prescriptions increased from 3.9% in 2000 to 13.1% in 2015
- Diclofenac prescriptions decreased from 16.2% in 2000 to 2.5% in 2015
- Celecoxib prescriptions increased from 0.6% in 2000 to 8.8% in 2004
- Codeine prescriptions increased from 3.2% in 2000 to 5.0% in 2005
- Mean treatment duration for tramadol was 22 (5 – 67) days
- No statistically significant difference in all-cause mortality observed between tramadol and codeine (519 deaths or 32.2/1000 person-years vs 552 deaths or 34.6/1000 person-years)
- HR 0.94
- 95% CI 0.83 – 1.05
Strengths:
- Large cohort of patients
- Only 6% of enrolled participants were unenrolled from a GP practice participating in THIN
- 6 sensitivity analyses were performed to assess robustness of study findings
Limitations:
- Why one drug was prescribed over another cannot be known from this study due to its retrospective nature
- Unclear of all other medications patients were taking
- There was a downtrend in the number of prescriptions of some NSAIDs, while there was a dramatic increase in tramadol prescriptions during the same time period
- Even though there was a sensitivity analysis, there is no way to ensure patients were compliant with medications as this was data recorded from a database
- Mortality rates from cardiovascular, gastrointestinal, infection, cancer, and respiratory diseases were higher in the tramadol group compared to NSAIDs. However, due to the small number of deaths from each specific cause, most associations were not statistically significant
- Patients in the tramadol cohort were older, had a higher BMI, longer duration of osteoarthritis, higher prevalence of comorbid disease, other prescriptions, and health care utilization than NSAIDs in the unmatched analysis. The authors tried to compensate for this by propensity matching to ensure balance between groups. However, this makes the results susceptible to confounding by indication (i.e. distortion that modifies an association between an exposure and an outcome, caused by the presence of an indication for the exposure that is the true cause of the outcome). It is possible that some participants were experiencing pain from undetected early-stage cancer and therefore given stronger pain medications
- This study links an association of tramadol to mortality, but does not by itself show causation
- 4 – 29.7% of causes of death were not known, small number of cause-specific deaths, did not allow for study to have adequate statistical power to evaluate the relationship of tramadol to cause-specific mortality
- Study conducted among patients with OA and therefore findings may not be generalizable to patients with other diseases
Discussion:
- The exact mechanism linking tramadol to mortality is unclear. Some plausible explanations include postoperative delirium, respiratory depression (especially with consumption of alcohol or other CNS depressants), hypoglycemia, hyponatremia, fractures, or falls
Author Conclusion: “Among patients aged 50 years and older with osteoarthritis, initial prescription of tramadol was associated with a significantly higher rate of mortality over 1 year of follow-up compared with commonly prescribed nonsteroidal anti-inflammatory drugs, but not compared with codeine. However, these findings may be susceptible to confounding by indication, and further research is needed to determine if this association is causal.”
Clinical Take Home Point: Despite this study being a large cohort of patients, its retrospective nature and bias toward more comorbid conditions in the tramadol group, makes it difficult to draw any definitive conclusions about the association between tramadol and one year all-cause mortality. However, given tramadol’s multiple side effects, potential drug-drug interactions, and lack of consistent pain control, this study with all its methodological issues does not change my own practice or bias of calling tramadol…tramadont. Using tramadol as a first line agent for OA does not make sense.
References:
- Zeng C et al. Association of Tramadol With All-Cause Mortality Among Patients with Osteoarthritis. JAMA 2019. PMID: 30860559
For More Thoughts on This Topic Checkout:
- David Juurlink at Tox and Hound (EMCrit): Tramdont
- Justin Morgenstern at First10EM:
Post Peer Reviewed by: Anand Swaminathan, MD (Twitter: @EMSwami)
The post Tramadol or Tramadont appeared first on REBEL EM - Emergency Medicine Blog.