
 I recently gave a talk on the initial management of trauma patients with hemorrhagic shock. In the initial management of trauma resuscitation there are 4 key principles that should be followed:
I recently gave a talk on the initial management of trauma patients with hemorrhagic shock. In the initial management of trauma resuscitation there are 4 key principles that should be followed:
- Control bleeding
- Restore tissue perfusion
- Minimize iatrogenic injury from resuscitation itself
- Promote hemostasis
In this blog post I will summarize the lecture and the evidence for each of these principles…
MINIMIZE IATROGENIC INJURY
- PERMISSIVE HYPOTENSION
- Maintaining a lower blood pressure than physiologic levels in patients suffering from hemorrhagic blood loss/shock
- Dutton RP et al. J Trauma 2002 [1]
- 110 trauma patients with hemorrhagic shock were randomized to two resuscitation protocols: Target SBP >100mmHg vs Target SBP > 70mmHg
- There was no difference in mortality regardless of which target SBP patients were randomized too
- My best guess for target SBP goal in trauma patients with hemorrhagic shock would be 70 to 90mmHg (Excluding patients with TBI)
- By having a set goal you get what’s called cyclic hyper-resuscitation (SEE IMAGE BELOW)
- Low BP or MAP –> Aggressive Resuscitation –> Nl/High BP or MAP –> Low BP
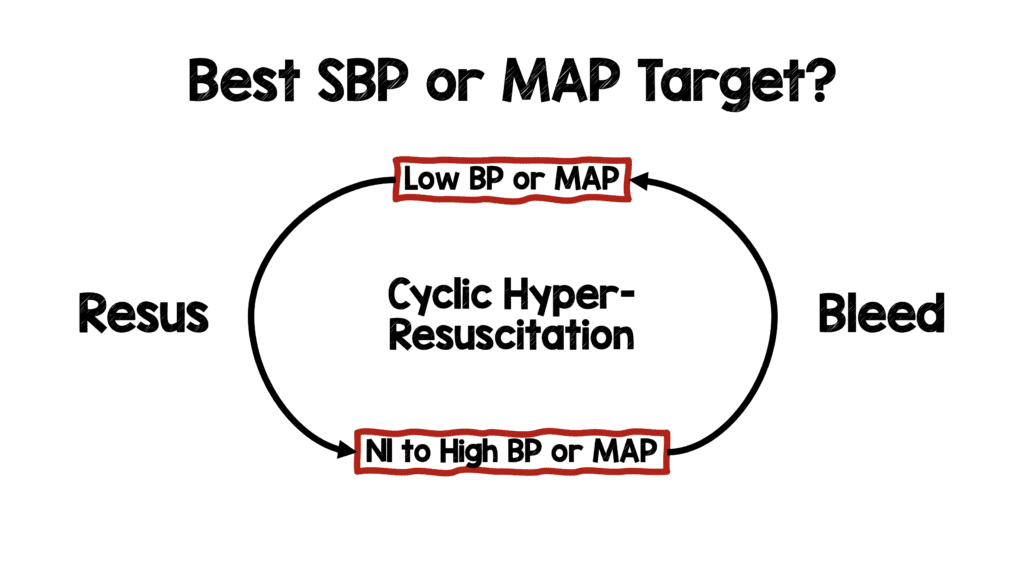
- Clinical Take Home: Targeting physiologic markers of perfusion (i.e. mental status, urine output, capillary refill) is more important than an actual goal
- PERMISSIVE HYPOTENSTION IN PTS WITH TBI
- Brotfain E et al. Shock 2012 [5]
- 48 rats given TBI and hypovolemic shock
- Resuscitation goals included MAP target of 80, 100, and 120mmHg at 15min
- The group with the highest MAP target had the largest amount of resuscitation
- Neurological outcomes and mortality were inversely correlated with aggressiveness of resuscitation (MAP target of 80mmHg provided the best results)
- Spaite DW et al. Ann Emerg Med 2017 [6]
- This was a retrospective database review of 7521 traumatic brain injury patients
- SBP target ≥90mmHg resulted in a mortality of 7.8% vs SBP target <90mmHg which resulted in a mortality of 33.4%
- Clinical Take Home Point: In patients with TBI and hypovolemic shock, target a SBP or MAP ≥90mmHg, but know this is based on limited evidence.
- Brotfain E et al. Shock 2012 [5]
- CRYSTALLOIDS
- Too much crystalloid resuscitation in traumatic hemorrhagic shock can increase dilutional coagulopathy, as well as increase morbidity and mortality
- Bickell WH et al. NEJM 1994. [2]
- Prospective trial comparing immediate vs delayed fluid resuscitation in 598 adult patients with penetrating torso injuries presenting with a pre-hospital SBP ≤90mmHg
- Immediate fluid resuscitation had a higher mortality, more complications and longer hospital length of stay
- Clinical Take Home Point: Crystalloid fluid resuscitation can be counterproductive and delay of aggressive crystalloid fluid resuscitation until hemorrhage control is achieved improves outcomes (If blood products not available consider small volume crystalloid boluses (i.e. 250 cc) up to 1L)
- VASOPRESSORS
- Current dogma is that vasopressors are not helpful in trauma patients as they can worsen ischemia (no reason to squeeze the pipes if the tank is empty).
- Richards JE et al. Anesth Analg 2021 [3]
- This was a narrative review article
- Concluded that the pathophysiology of shock in trauma patients is complex
- Initial sympathoexcitatory phase: Attempt to compensate for acute blood loss and characterized by vasoconstriction, tachycardia, and preserved MAP
- Subsequently a sympathoinhibitory vasodilation phase occurs: Leads to hypotension
- Resuscitation of traumatic shock needs to target an appropriate balance with intravascular volume and vascular tone
- Sims et al. JAMA Surg 2019 [4]
- The AVERT-Shock Trial
- Only RCT in human trauma patients with vasopressors to date
- Randomized, double-blind, placebo-controlled clinical trial of 100 adult trauma patients having received at least 6U of any blood product within 12hrs of injury
- Randomized to: After administration of a vasopressin bolus (4U) vs placebo, pts received vasopressin (0 to 0.04U/min) or placebo for 48hrs to maintain a MAP of at least 65mmHg
- Vasopressin was only given after definitive hemorrhage control was achieved
- The use of vasopressin resulted in less blood products at 48 hrs (1.7 vs 3U) but no difference in mortality (Study not powered for this outcome)
- Clinical Take Home Point: The use of vasopressors is controversial and requires a nuanced approach
SUMMARY OF MINIMIZING IATROGENIC INJURY
RESTORE PERFUSION
- VOLUME REPLACEMENT
- Blood Products >>> Crystalloids
- Holcomb JB et al. JAMA 2015 [7]
- The PROPPR Trial
- 680 severely injured adult trauma patients
- Patients randomized to Plasma, Platelets, and PRBCs in a 1:1:1 ratio vs 1:1:2 ratio
- No difference in overall mortality at 24 hrs BUT 1:1:1 achieved hemostasis faster and fewer experienced death due to exsanguination at 24hrs
- Crombie N et al. Lancet Haematol 2022 [8]
- The RePHILL Trial
- 432 adult trauma patients with trauma related hemorrhagic shock and hypotension (defined as SBP <90mmHg or absense of radial pulse) resuscitated with pre-hospital blood products
- Patients randomized to PRBCs/Lyophilised plasma vs saline solution
- Trial recruitment was stopped prior to intended sample size or 490 patients due to COVID-19 pandemic
- Composite primary outcome was mortality, impaired lactate clearance or both
- No difference in composite primary outcome
- Reasons why trial may have been negative
- Mostly blunt trauma patients (not penetrating injuries)
- Transport times were short for many patients
- Better resuscitation pre-hospital (Sicker patients getting to the hospital which could drive up mortality overall)
- Clinical Take Home Point: Current evidence shows plasma, platelets, PRBCs in a 1:1:1 ratio is best strategy for resuscitation of trauma patients with hemorrhagic shock
- MASSIVE TRANSFUSION PROTOCOL (MTP)
- Who Needs a MTP?
- ABC Score:
- Penetrating Mechanism
- SBP ≤90mmHg
- HR ≥120 BPM
- Positive FAST Abdominal Views
- If ≥2 present, consider MTP
- RABT Score
- Revised Assessment of Bleeding and Transfusion Score
- Penetrating Injury
- Positive FAST
- Shock Index >1.0
- Pelvic Fracture
- A score ≥2 present, consider MTP
- Clinical Take Home Point: Use of balanced transfusion (including PRBCs and clotting factors) helps avoid dilutional coagulopathy
- ABC Score:
- Who Needs a MTP?
- WHOLE BLOOD VS COMPONENT THERAPY
- Kronstedt S et al. Cureus 2022 [9]
- Narrative Review
- Whole blood logistically makes sense but thus far mostly small prospective or retrospective studies have failed to demonstrate a significant benefit of whole blood vs blood component therapy
- Clinical Take Home Point: Current literature suggests that whole blood therapy shows promise as a treatment strategy for adult trauma patients
- Kronstedt S et al. Cureus 2022 [9]
SUMMARY OF RESTORING PERFUSION
PROMOTE HEMOSTASIS
- TRANEXAMIC ACID (TXA)
- CRASH-2 Trial Collaborators et al. Lancet 2010 [10]
- >20,000 adult trauma patients with SBP <90mmHg
- Patients randomized to TXA 1g over 10 min + 1g IV over 8hrs vs Placebo given within 8hrs of injury
- In-hospital mortality by 28d reduced (14.5% vs 16%; ARR 1.5%; NNT = 67)
-
Clinical Take Home Point:
- TXA 1g over 10 min + 1g IV over 8 hrs reduces the risk of death in bleeding trauna patients when given within 3hrs of injury
- TXA given as a 2g bolus (Single bolus easier to remember than giving two doses; No evidence of harm)
- CRASH-3 Trial Collaborators et al. Lancet 2019 [11]
- >12,000 Adults with TBI within 3hrs of injury, GCS ≤12 or any ICH on CT scan, and no major extracranial bleeding were eligible
- Patients randomized to TXA 1g over 10 min + 1g IV over 8hrs vs Placebo given within 8hrs of injury (Later amended to within 3hrs of injury)
- Patients randomized to TXA 1g over 10 min + 1g IV over 8hrs vs Placebo
- Primary outcome of head injury-related death within 28 days was the primary outcome (NO DIFFERENCE)
- Risk of head injury-related death in patients with mild-to-moderate head injury (GCS 9 to 15) was reduced but not in patients with severe head injury (GCS 3 to 8)
- Clinical Take Home Point: TXA didn’t benefit in the primary outcome of head injury-related death within 28 days, but the authors had to narrow down the group to get a significant benefit making it more difficult to apply the results to all TBI patients
- CRASH-2 Trial Collaborators et al. Lancet 2010 [10]
- CRYOPRECIPITATE
- Curry N et al. British Journal of Anaesthesia 2015 [12]
- CRYOSTAT-1 trial
- Unblinded feasibility RCT
- 202 Adult trauma patients requiring MTP
- 85% got cryoprecipitate within 90min
- No difference in 28d all cause mortality
- Clinical Take Home Point: It is feasible to administer cryo within 90min of admission to hospital
- CRYOSTAT-2 Trial
- Pending Publication
- Curry N et al. British Journal of Anaesthesia 2015 [12]
- LABS TO FOLLOW
- PLATELETS
- Target >50,000
- If head injury suspected or ICH target >100,000
- INR
- Target INR <2
- FIBRINOGEN
- Target 150 to 1000mg/dL
- 10U Cryoprecipitate ≈75mg/dL
- CALCIUM
- Citrate in blood products dilutes out calcium
- Calcium also augments clot formation
- 1 to 2g CaCl or 3 to 6g CaGluc for every 6U of blood products
- 1amp of CaCl = 3amps of CaGluc (1 to 3 ratio)
- PLATELETS
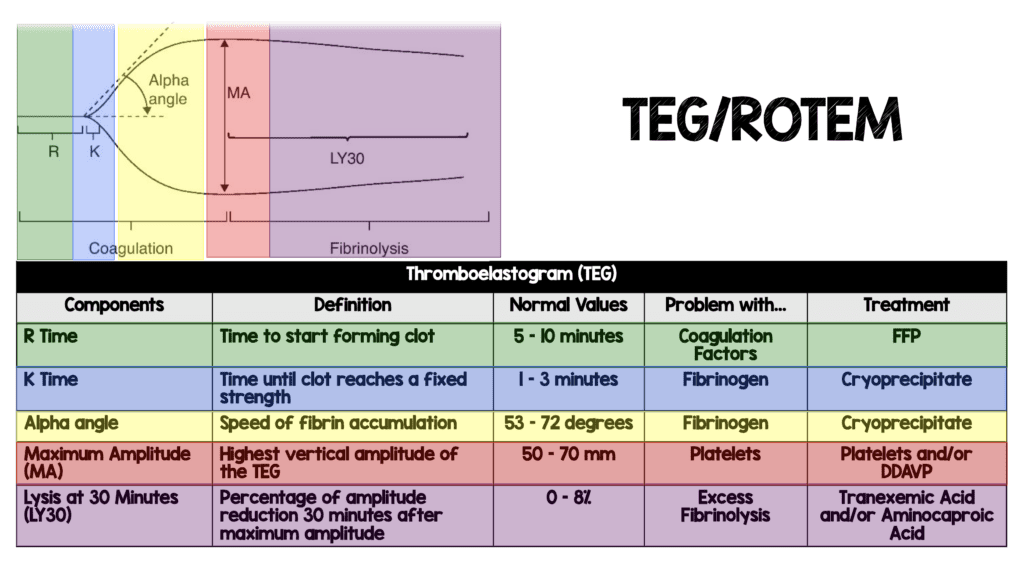
- TEG/ROTEM
-
- Badsaas-Aasen K et al. Intensive Care Med 2020. [13]
- ITACTIC Trial
- 480 Adult trauma patients getting MTP augmented by Viscoelastic Hemostatic Assays vs Conventional Coagulation Tests
- No difference in proportion of patients alive and free of massive transfusion at 24hrs after injury
- Major flaw of study is many patients did not develop coagulopathy in this study
- Clinical Take Home Point: Blood products are given so rapidly during resuscitation that it’s practically impossible to use standard labs to guide product administration (By the time a set of labs has returned, it is already obsolete). Not every institution will have TEG/ROTEM and more evidence is needed to support or refute its use
- Badsaas-Aasen K et al. Intensive Care Med 2020. [13]
- 4F-PCC
- Bouzat P et al. JAMA 2023 [14]
- PROCOAG Trial
- 324 trauma patients receiving standard trauma resuscitation management at risk of needing MTP randomized to 4F-PCC vs placebo
- No difference in the median 24hr blood product consumption (primary outcome)
- Way more thromboembolic events in the 4F-PCC group (35% vs 24%)
- Clinical Take Home Point: The addition of 4F-PCC does not result in decreased blood product consumption compared to placebo and resulted in a higher rate of thromboembolic events. At this time the use of 4F-PCC is not supported in patients with trauma at risk of MTP
- Bouzat P et al. JAMA 2023 [14]
SUMMARY OF PROMOTING HEMOSTASIS
CONTROL BLEEDING
- STRATEGY
- Use the fastest strategy to get hemorrhage control
- Tourniquets
- Direct Pressure
- Packing
- Sutures
- Interventional Surgical Repair
- Definitive Surgical Repair
- Be systematic in finding bleeding (SCALPER)
- S = Scalp
- C = Chest
- A = Abdomen
- L = Long Bones
- P = Pelvis
- E = Extremities
- R = Retroperitoneum
- Use the fastest strategy to get hemorrhage control
- TOURNIQUETS
- Schroll R et al. J Trauma Acute Surg 2022 [15]
- Multicenter prospective observational trial
- ≈1400 adult patients with extremity trauma injuries requiring a trauma center
- Patients either received prehospital tourniquets or no tourniquets
- Tourniquets controlled bleeding in 87.7% of injured limbs
- Tourniquet patients were less likely to arrive in shock compared to no torniquets (13.0% vs 17.4%)
- No difference in limb complications
- Clinical Take Home Point: Tourniquets result in decreased incidence of shock without an increase in limb complications
- Schroll R et al. J Trauma Acute Surg 2022 [15]
- CHEST TUBES
- Kulvatunyou N et al. J Trauma acute Care Surg 2021 [16]
- Non-inferiority randomized trial of 120 patients randomized to 14Fr pigtail vs 28 to 32Fr chest tube for traumatic hemothorax (Patients were all hemodynamically stable)
- No difference in failure rate
- Inferiority margin of 15% is very wide making it easier to show non-inferiority
- Additionally, this seems to be a convenience sample (i.e. patients were hand picked)
- Clinical Take Home Point: In selected hemodynamically stable trauma patients with hemothorax the use of 14Fr pigtail catheters appear to have drainage rates and complication rates that are at least equal and your patient will thank you for using a smaller tube
- Kulvatunyou N et al. J Trauma acute Care Surg 2021 [16]
- REBOA
- Joseph B et al. JAMA Surg 2019 [17]
- Retrospective case-control analysis of 140 adult trauma patients undergoing REBOA
- Looked at mortality in the ED, 24hrs, and after 24hrs
- There was a higher 24hr mortality, rate of AKI, and rate of lower limb amputation in the REBOA group compared to standard care
- Additionally, there was a longer time to interventional radiology angioembolization or laparotomy in the REBO group
- Clinical Take Home Point: Currently at some institutions REBOA is still being used in non-compressible torso trauma, but more evidence is needed before adoption into standard practice
- Cralley AL et al. JAMA Surg 2022 [18]
- Prospective multicenter comparative effectiveness study from the Aortic Occlusion for Resuscitation in Trauma and Acute Care Surgery (AORTA) Registry
- Performed propensity score matching and subgroup multivariate analysis to control for confounders
- Aorta occlusion via REBOA zone 1 (above celiac artery) vs Resuscitative thoracotomy
- Primary outcome was survival
- 991 patients included
- Propensity score matching selected 112 comparable patients (56 pairs)
- REBOA zone 1 aortic occlusion was associated with a statistically significant lower mortality compared with resuscitative thoracotomy (78.6% vs 92.9%)
- Multivariate analysis confirmed survival benefit of REBOA zone 1 after adjustment for significant confounders (RR 1.25; 95% CI 1.15 to 1.36)
- In all subgroup analyses (Cardiopulmonary resuscitation on arrival, traumatic brain injury, chest injury, pelvic injury, blunt/penetrating mechanism, SBP ≤60mmHg on Aortic occlusion injury) REBOA zone 1 offered an either similar or superior survival
- Clinical Take Home Point: REBOA zone 1 aortic occlusion was associated with a better or similar survival than resuscitative thoracotomy. This study establishes a clinical equipoise between the above two resuscitation strategies to justify the planning of a randomized controlled trial to evaluate safety and effectiveness of REBOA zone 1 aortic occlusion in trauma resuscitation
- Joseph B et al. JAMA Surg 2019 [17]
SUMMARY OF BLEEDING CONTROL
As stated at the top of this post, this is simply a summary of the best current evidence in initial trauma resuscitation. In the initial management of trauma patients there are 4 key principles that should be followed:
- Control bleeding
- Restore tissue perfusion
- Minimize iatrogenic injury from the resuscitation itself
- Promote hemostasis
References:
- Dutton RP et al. Hypotensive resuscitation during active hemorrhage: impact on in-hospital mortality. J Trauma. 2002. PMID: 12045644
- Bickell WH et al. Immediate Versus Delayed Fluid Resuscitation for Hypotensive Patients with Penetrating Torso Injuries. NEJM 1994. PMID: 7935634
- Richards JE et al. Vasopressors in Trauma: A Never Event? Anesth Analg 2021. PMID: 33908898
- Sims et al, “Effect of Low-Dose Supplementation of Arginine Vasopressin on Need for Blood Product Transfusions in Patients With Trauma and Hemorrhagic Shock: A Randomized Clinical Trial,” JAMA Surg, Aug. 2019. PMID: 31461138
- Brotfain E et al. Severe Traumatic Brain Injury and Controlled Hemorrhage in Rats: Quest for the Optimal Mean Arterial Blood Pressure After Whole Fresh Donor Blood Resuscitation. Shock 2012. PMID: 23143053
- Spaite DW, Hu C, Bobrow BJ, et al. Association of out-of- hospital hypotension depth and duration with traumatic brain injury mortality. Ann Emerg Med. 2017. PMID: 28559036
- Holcomb JB et al. Transfusion of Plasma, Platelets, and Red Blood Cells in a 1:1:1 vs a 1:1:2 ratio and Mortality in Patients with Severe Trauma: The PROPPR Randomized Clinical Trial. JAMA 2015. PMID: 25647203
- Crombie N et al. Resuscitation with Blood Products in Patients with Trauma-Related Haemorrhagic Shock Receiving Prehospital Care (RePHILL): A Multicentre, Open-Label, Randomised, Controlled, Phase 3 Trial. Lancet Haematol 2022. PMID: 35271808
- Kronstedt S et al. The Role of Whole Blood Transfusions in Civilian Trauma: A Review of Literature in Military and Civilian Trauma. Cureus 2022. PMID: 35481238
- CRASH-2 trial collaborators, Shakur H, Roberts I, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet (London, England). 2010; 376(9734):23-32.PMID: 20554319
- The CRASH-3 Trial Collaborators. Effects of Tranexamic Acid on Death, Disability, Vascular Occlusive Events and Other Morbidities in Patients with Acute Traumatic Brain Injury (CRASH-3): A Randomised, Placebo-Controlled Trial. Lancet 2019. PMID: 31623894
- Curry N et al. Early Cryoprecipitate for Major Haemorrhage in Trauma: A Randomised Controlled Feasibility Trial. British Journal of Anaesthesia 2015. PMID: 25991760
- Badsaas-Aasen K et al. Viscoelastic Haemostatic Assay Augmented Protocols for Major Trauma Haemorrhage (ITACTIC): A Randomized, Controlled Trial. Intensive Care Med 2020. PMID: 33048195
- Bouzat P et al. Efficacy and Safety of Early Administration of 4-Factor Prothrombin Complex Concentrate in Patients with Trauma at Risk of Massive Transfusion: The PROCOAG Randomized Clinical Trial. JAMA 2023. PMID: 36942533
- Schroll R et al. AAST Multicenter Prospecitve Analysis of Prehospital Tourniquet Use for Extremity Trauma. J Trauma Acute Care Surg 2022. PMID: 35609289
- Kulvatunyou N et al. the Small (14Fr) Percutaneuos Catheter (P-CAT) Versus Large (28 – 32Fr) Open chest Tube for Traumatic Hemothorax: A Multicenter Randomized Clinical Trial. J Trauma Acute Care Surg. 2021. PMID: 33843831
- Joseph B et al. Nationwide Analysis of Resuscitative Endovascular Balloon Occlusion of the Aorta in Civilian Trauma. JAMA Surgery 2019. PMID: 30892574
- Cralley AL et al. Zone 1 Endovascular Balloon occlusion of the Aorta vs resuscitative Thoracotomy for Patient Resuscitation After Severe Hemorrhagic Shock. JAMA Surg 2022. PMID: 36542395
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)
The post Trauma Resuscitation Updates appeared first on REBEL EM - Emergency Medicine Blog.