

A 25-year-old man presents with 6 hours of penile pain and swelling after recreational penile injection of Trimix (alprostadil, papaverine, and phentolamine). He denies any history of sickle cell disease or penile trauma. On exam, he is in moderate discomfort and has a tumescent penis with a soft glans. You suspect the patient is suffering from ischemic, low-flow priapism. Manual compression and ice application have been attempted with no significant improvement in the patient’s clinical status.
Trick of the Trade: Penile decompression using 16-gauge angiocatheter
Equipment:
- 27-gauge needle w/ 1.75” length (for dorsal penile nerve block)
- 20 – 30 mL lidocaine 1% without epinephrine (for dorsal penile nerve block)
- 16-gauge IV catheter (acquire these from your trauma/needle decompression supply)
- 10 mL syringe
- 20 mL syringe
- Phenylephrine (“neo-stick”) 100mcg/1mL (typically in 10 mL syringe)
- Urinal or basin
- 4×4 sterile gauze stack
- sterile towels
- sterile gloves
- povidone-iodine
Technique:
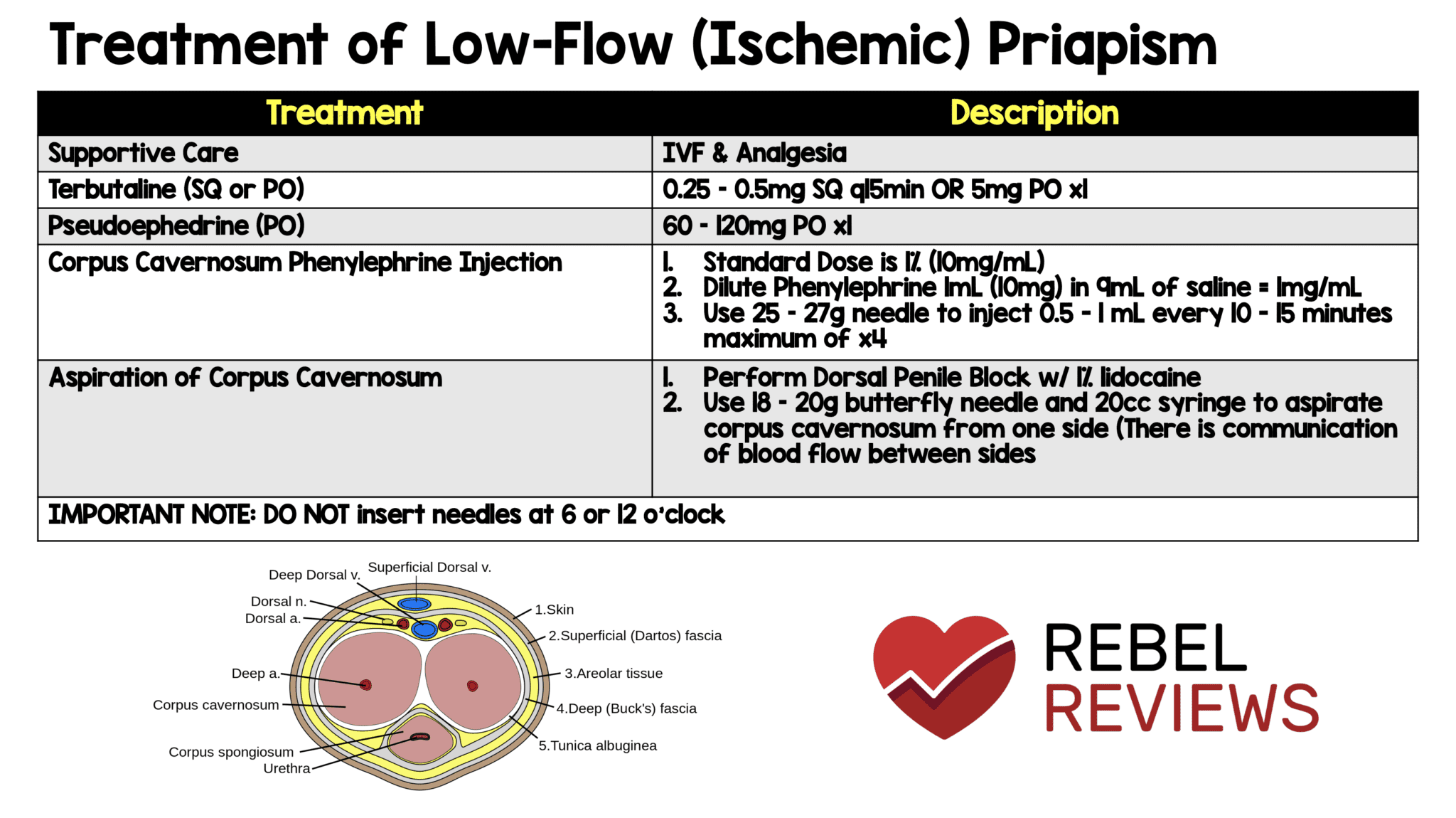
- Review penile anatomy: The dorsal nerve, arteries, and vein run along the dorsal aspect of the penis in its erect position. The corpus cavernosa flank this bilaterally. The unpaired corpus spongiosum lies on the volar side; the urethra runs through this structure.

Image 1: A review of the anatomy to demonstrate the corpus cavernosa in relation to the dorsal nerve/arteries/vein and the opposing corpus spongiosum, where the urethra is located.
- Offer parenteral pain control and/or sedation prior to the dorsal penile nerve block.
- Dorsal penile nerve block:
- Apply povidone-iodine generously to the penis shaft and base.
- Set up your sterile towels around the base of the penis.
- Similar to regional/ring digital nerve blocks, insert the needle at the dorsal base of the penis toward the pubic bone (1, in the image below).
- Fan needle outward to distribute lidocaine evenly (2 and 3, in the image below).

Image 2: For adequate penile nerve block, lidocaine is injected at numbered points 1, 2, and 3.
- Stabilize the handling of the genitalia with a 4×4 gauze wrapped around the tip of the penis. This is helpful when the iodine solution is still wet, or when blood gets on the shaft.
- At a 90 degree angle to the skin, insert a 16-gauge angiocatheter at the 3 o’clock and/or 9 o’clock position close to the base of the penis.
- The corpus cavernosa are vascularly connected, so a single catheter inserted on either side of the penis should be able to access both sections.
- The degree of coagulation can determine or influence the decision to use one or two entries.
- Bilateral aspiration is not always required, although it may help accelerate drainage, especially if blood has begun coagulating in delayed presentations.
- Lateral entry points provide the safest approach to avoid urethral injury.
- The degree of coagulation can determine or influence the decision to use one or two entries.
- The corpus cavernosa are vascularly connected, so a single catheter inserted on either side of the penis should be able to access both sections.
- Advance the needle until you see a flash of blood.

Image 3: A plastic angiocatheter stabilized in the corpus cavernosum.
- Withdraw the needle, leaving the plastic IV catheter in place.
- Avoid crossing the midline to prevent injury to vascular structures.
- There should be a steady flow of blood that can be absorbed by 4×4 gauze pads or drain directly into the urinal
- Initially, dark venous blood will flow. A change into bright arterial blood is a marker for success [1].

Image 4: For more rapid drainage, or patients in which significant coagulation is anticipated, bilateral drainage is appropriate.
- Consider sending a blood sample from the catheter for gas analysis if there is a question regarding arterial or venous shunting.
- Gases with hypoxia, hypercarbia, and acidosis are indicative of ischemic (veno-occlusive, low flow) priapism [1].
- Normalization of the cavernosum blood gas also supports the resolution of ischemic priapism [1].
- As the rate of blood flow diminishes, firm manual pressure can be applied to decompress the corpus.
- Alternatively, with the same angiocath in place, irrigate with 10 mL aliquots of normal saline through the catheter to promote hemolysis of clotted blood, then aspirate through either side. A 10 mL or 20 mL syringe can be used to aspirate. Minimize multiple approaches; this can lead to the development of a hematoma.
- If complete detumescence is not achieved with passive drainage, manual decompression, aspiration, and saline irrigation, small infusions of vasoactive sympathomimetics (alpha-agonists) can be used. Depending on the concentration of phenylephrine available, administer 100 – 500 mcg/mL in 1 mL aliquots every 3-5 minutes while monitoring for detumescence; this can be repeated for an hour [1,2].
- Intracavernosal injection of phenylephrine can have systemic effects, so it is important to keep patients on the monitor to observe for severe hypertension, reflex bradycardia, or other dysrhythmias.

Image 5: Commonly available phenylephrine dose, to be administered in 1 mL aliquots.
- Urgent urology consultation is recommended, especially if there is a failure to achieve detumescence with the techniques above, as the patient may require corpus cavernosum-spongiosum shunting. Any delays in definitive treatment increase long term, permanent nerve injury, potentially resulting in impotence.
Patient Selection:
This technique can be attempted in any patient presenting with ischemic (low-flow) priapism not responsive to supportive measures (compression/ice).
Caution:
Do not insert needles at 6 or 12 o’clock. The neurovascular bundle runs along the dorsal aspect of the penis at 12 o’clock, and the urethra runs along the ventral aspect at 6 o’clock. Staying along the lateral aspects of the penis at 3 and 9 o’clock helps to avoid injuring these structures.
Discussion:
Check out RebelEM’s helpful pharmaceutical review of priapism.
What do you think about this technique? Any more pearls or suggestions?
Check out more ALiEM Tricks of the Trade.
References:
- Montague DK, Jarow J, Broderick GA, Dmochowski RR, Heaton JPW, Lue TF, et al. Guideline on the management of priapism. American Urological Association. Available at: https://www.auanet.org/guidelines/priapism-(2003-reviewed-and-validity-confirmed-2010)>. 2010; Accessed: April 15, 2020
- Davis JE, Silverman MA. Urologic Procedures. In: Roberts and Hedges’ Clinical Procedures in Emergency Medicine and Acute Care. 7th ed. Philadelphia, PA: Elsevier; 2019:1141-1185.
Author information

The post Trick of the Trade: Angiocatheter for manual aspiration of priapism appeared first on ALiEM.

{kind=link}