
 Ear, nose, and throat (ENT) complaints are commonly seen in the emergency department. When you hear “ENT emergencies,” you probably think about epistaxis, sinusitis, and possibly foreign body removal (either from the ear or nose). While not as common, auricular hematomas are equally important to both understand and know how to manage. As a former wrestler, I can attest to the importance of 1) knowing how to accurately diagnose and 2) how to treat this injury to prevent future development of “cauliflower ear”.
Ear, nose, and throat (ENT) complaints are commonly seen in the emergency department. When you hear “ENT emergencies,” you probably think about epistaxis, sinusitis, and possibly foreign body removal (either from the ear or nose). While not as common, auricular hematomas are equally important to both understand and know how to manage. As a former wrestler, I can attest to the importance of 1) knowing how to accurately diagnose and 2) how to treat this injury to prevent future development of “cauliflower ear”.
An auricular hematoma is a collection of blood underneath the perichondrium of the ear that typically occurs secondary to trauma. Common mechanisms of injury include an ear-piercing gone wrong or blunt trauma in contact sports (wrestling, boxing, and martial arts). Inadequate treatment of an auricular hematoma can lead to the development of an auricular deformity commonly known as “cauliflower ear,” which develops from permanent cartilage destruction.
Diagnosis
This is commonly done with physical examination alone, but if there is a concern for inner ear/skull injury, you may consider obtaining a CT scan to evaluate for skull fractures, etc. Ultrasound could also be used in the presence of an old injury to evaluate for an acute fluid collection. If there is overt erythema and swelling that extends beyond the pinna of the ear, you should consider the development of perichondritis, an infection of the perichondrium that may require antibiotics. If there is concomitant hearing loss or hearing issues, other diagnoses should be considered.
Treatment
Auricular hematomas are treated by either needle aspiration or incision and drainage. Both techniques should be performed under sterile conditions after adequate analgesia with either a regional auricular block or local infiltration. Regardless of which technique you choose, hematoma evacuation should be followed by the placement of a bolster dressing to eliminate the potential for fluid reaccumulating.
Needle Aspiration
Indications: small, acute hematomas; specifically, hematomas < 2 cm in diameter and present for less than 48 hours
How To Perform: Clean and prep the skin. Anesthetize the area either with an auricular block or skin wheal of local anesthetic. Identify and aspirate the most fluctuant part of the hematoma with an 18 gauge needle while milking the hematoma to ensure complete drainage. Apply manual pressure to the area of the evacuated hematoma for 3-5 minutes.

Incision and Drainage
Indications: auricular hematomas ≥ 2cm in diameter, all hematomas present from 48 hours up to 7 days, hematomas that reaccumulate after needle aspiration
How To Perform: Clean and prep the skin. Perform an auricular block to achieve analgesia. Incise the auricular skin overlying the hematoma using an #11 or #15 blade. Incising along the most superior aspect of the hematoma allows for better cosmetic healing as the scar will be concealed by the superior aspect of the helix. The incision should be adequate to drain the clotted blood completely, but no longer than 1cm. Use a curved hemostat to help break up the remaining clot and milk the hematoma to ensure complete drainage. Irrigate with sterile saline. Apply manual pressure to the area of the evacuated hematoma for 3-5 minutes.
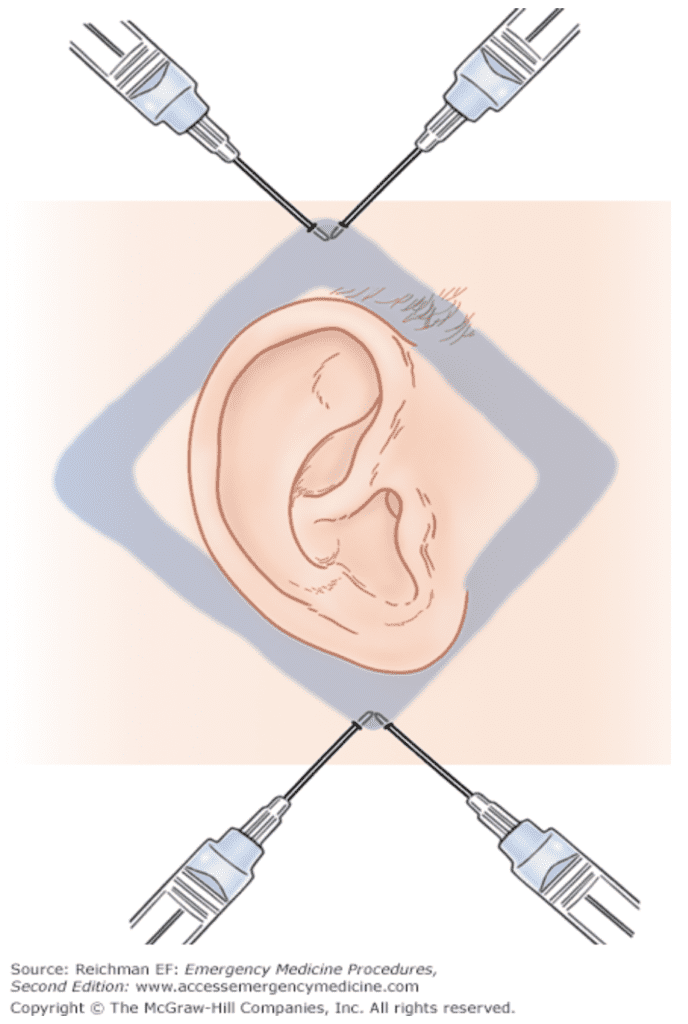 Auricular Block
Auricular Block
Cleanse the ear and surrounding skin with an antiseptic solution. Enter the skin at a point just below the ear and advance the needle posteriorly along the skin over the mastoid behind the ear. Inject up to 5mL of Lidocaine as the needle is withdrawn. Without removing the needle from the skin, redirect it anterior to the ear and inject up to 5mL of Lidocaine again. The tracks should form an upright “V”. Next enter the skin at a point just above the ear and advance the needle posteriorly behind the ear. Inject up to 5mL of Lidocaine as the needle is withdrawn. Without removing the needle from the skin, redirect it anterior to the ear and inject up to 5mL of Lidocaine again. The tracks should form an inverted “V”. Wait 10-15 minutes after completion of injections in order to achieve maximum anesthesia.
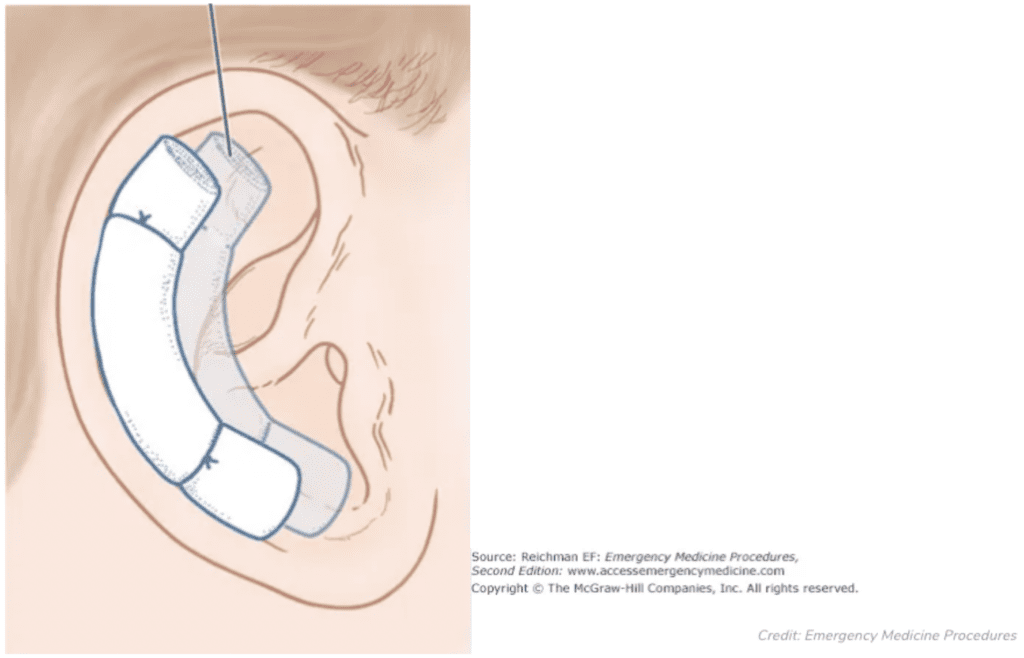
Sewn-In Bolster Dressing
Using 4-0 non-absorbable suture of your preference, pierce the pinna from anterior to posterior near the hematoma drainage site. Make a loop around a dental roll on the posterior aspect, then pierce the pinna from posterior to anterior. Place a second dental roll along the curvature of the helix over the drainage site on the anterior aspect. Tie your suture around the dental roll on the anterior aspect, cinching down the suture to bring the two dental rolls together to compress the auricle. Placing sutures over the superior and inferior portions of the dental rolls will help maintain the bolster dressing’s positioning. Bolster dressings typically remain in place for 7-10 days.
Disposition
Patients should be referred for Otolaryngology follow up as they 1) may need additional evacuations, and 2) may need skin grafts if cartilage destruction occurs.
While patients presenting with auricular hematomas are relatively few and far between for emergency medicine physicians, it is an injury well within our realm to properly treat.
Guest Post By:


Emergency Medicine Resident
OhioHealth/Doctors Hospital EM Residency
Resources:
- Johnston C et al. How to Treat an Auricular Hematoma in the Emergency Department. [Updated 2013 April 13]. EP Monthly. [Link is HERE]
- Krogmann RJ et al. Auricular Hematoma. [Updated 2018 Dec 16]. Stat Pearls. [Link is HERE]
- Reichman EF. Auricular Hematoma Evacuation. In: Reichman EF. eds. Reichman’s Emergency Medicine Procedures, 3e. McGraw-Hill; Accessed: April 2, 2019, 2020. [Link is HERE]
The post Auricular Hematoma Management appeared first on REBEL EM - Emergency Medicine Blog.