
 Background: Community acquired pneumonia (CAP), defined as lower bronchial tree infection in a patient that has not been hospitalized in the last 90 days is a commonly diagnosed disease. There are between 2-4 million episodes per year in the US with roughly 500,000 hospital admissions (Rosen’s). Most outpatients are treated with azithromycin (or another macrolide antibiotic) as this drug gives a simple treatment regimen (single drug, simple dosing, short course). However, the efficacy of this regimen has been questioned in recent years as resistance patterns shift.
Background: Community acquired pneumonia (CAP), defined as lower bronchial tree infection in a patient that has not been hospitalized in the last 90 days is a commonly diagnosed disease. There are between 2-4 million episodes per year in the US with roughly 500,000 hospital admissions (Rosen’s). Most outpatients are treated with azithromycin (or another macrolide antibiotic) as this drug gives a simple treatment regimen (single drug, simple dosing, short course). However, the efficacy of this regimen has been questioned in recent years as resistance patterns shift.
Article: Haran JP et al. Macrolide resistance in cases of community-acquired bacterial pneumonia in the emergency department. J Emerg Med 2018.
Common CAP Pathogens
- Typical Pathogens: S. pneumonia, H infuenzae
- Atypical Pathogens: Legionella, Mycoplasma, Chlamydophila
Rising Antibiotic Resistance
Emergency providers select empiric antibiotics based on the most likely pathogen (S. pneumonia most common overall, 22% by atypical pathogens (Arnold 2007)) without knowledge of the actual pathogen or exact resistances. Local resistance patterns can guide the selection. The 2007 Infectious Disease Society of America (IDSA)/American Thoracic Society (ATS) recommendations list macrolides as first line therapy for CAP but, they further specify that alternates should be considered when S. pneumonia resistance exceeds 25% (Mandell 2007). In vitro resistance rates currently exceed this threshold across all regions in the US.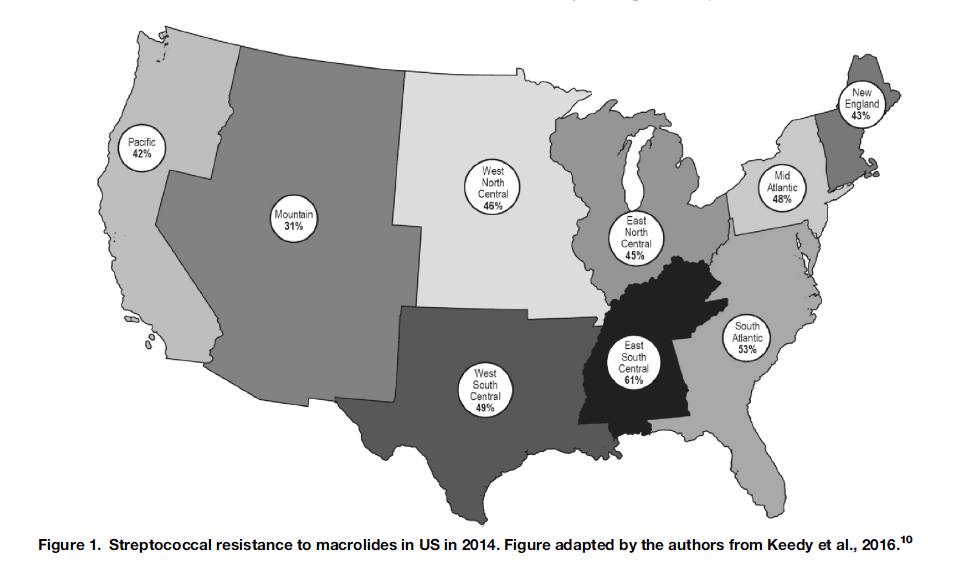
Although in vitro resistance does not directly correlate with in vivo resistance or treatment failure, it is used as a surrogate due to the difficulty in determining actual clinical failure.
Costs of Rising Resistance
Failure of outpatient treatment for CAP can result in a number of deleterious outcomes. While death is unlikely, hospitalization for treatment failure is common. Admission to the hospital or placement in an observation area for intravenous antibiotics is costly and can lead to iatrogenic harm. The benefit of admission appears to outweigh the harms in treatment failure but, this is unlikely to be true when treatment failure is due to the inadequacy of the antibiotic choice.
Alternative Approaches
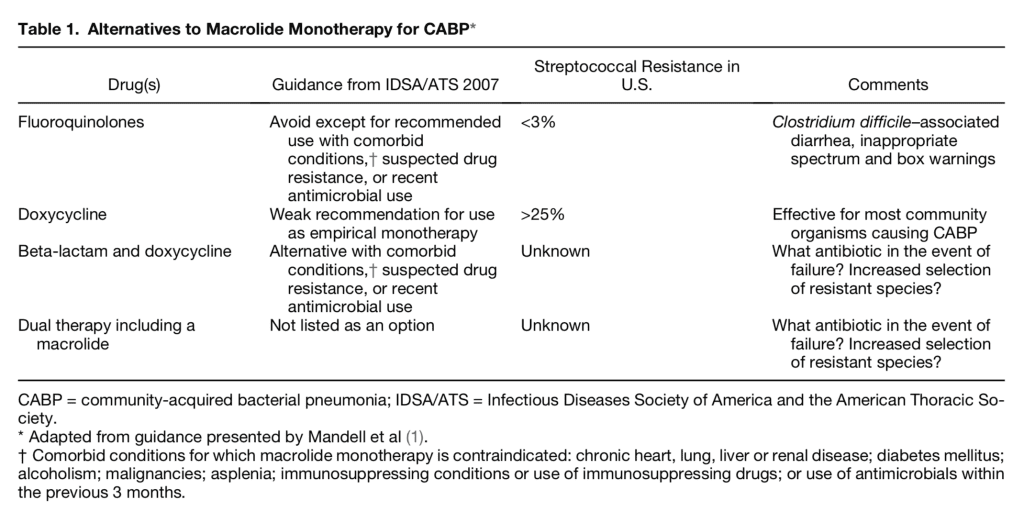
If macrolides should be avoided due to rising resistance patterns, we need to be aware of alternative options. The IDSA/ATS recommendations list three alternative treatment approaches for CAP:
Our Recommendations
Caveat: It is vital to check your local resistance patterns before embracing an alternate strategy.
I typically prescribe a beta-lactam (amoxicillin 500 mg Q6 X 7 days) + a macrolide (azithromycin 500 mg X 1 followed by 250 mg Q24 X 4 days). This combination is likely to cover both S. pneumoniae and the atypicals.
Rick Pescatore (Southern New Jersey) and Jenny Beck-Esmay (NYC) suggested that we can replace the amoxicillin with cefdinir 300 mg BID X 7 days.
Additionally, Rick and Salim (San Antonio, TX) note that the amoxicillin dose recommended by the IDSA is 1000 mg TID X 7 days though this was specifically recommended for patients with high-risk features, not your “run of the mill” CAP. Salim swaps out amoxicillin for amoxicillin/clavulanate 875/125 BID X 7 days in higher risk patients.
Doxycycline 100 mg Q12 X 7-10 days can be used as an alternative but due to increasing S. pneumoniae resistance, I reserve this for patients who have close follow up or, who I can see back in the ED in the next 2-3 days for clinical improvement. Failure of this approach would prompt me to add amoxicillin as above.
Rob Bryant and Caroline Vines (Intermountain, Utah) have a similar approach. Doxycycline is 1st line for them due to better susceptibility patterns for S. pneumonia. Azithromcyin + amoxicillin 1000 mg TID X 7 days as second line and fluoroquinolones (FQ) as 3rd line.
I typically avoid FQs secondary to their side effect profile but will consider using them in specific cases (I.e. severe penicillin allergy).
References
- Moran GJ, Talan, DA; Pneumonia, in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2010, (Ch) 76: p 978-89.
- Mandell LA et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007;44(Suppl 2):S27–72. PMID: 17278083
- Arnold FW et al. A worldwide perspective of atypical pathogens in community-acquired pneumonia. AmJ Respir Crit Care Med 2007;175:1086–93. PMID: 17332485
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie), Rob J. Bryant (Twitter: @RobJBryant13), Rick Pescatore (Twitter: @Rick_Pescatore), and Jenny Beck-Esmay (Twitter: @jbeckesmay)
The post Update in Community Acquired Pneumonia (CAP) Treatment: Macrolide Resistance appeared first on REBEL EM - Emergency Medicine Blog.