
 Background: Despite minimal high-quality supporting evidence (Seymour 2017, Liu 2017, Ferrer 2014, Sterling 2015), regulatory bodies have pushed for benchmark times for administration of antibiotics in patients with sepsis. While most clinicians would agree that in patients with septic shock antibiotics should be given as quickly as possible, the same does not hold true for those patients with less severe infections. In the US, the Centers for Medicare and Medicaid Services (CMS) currently mandates that antibiotics be started in patients within 3 hours of onset of new organ dysfunction in patients with systemic inflammatory response syndrome and documented infection. The Surviving Sepsis Campaign (SSC) has even more extreme recommendations stating that antibiotics should be started within 1 hour from triage in septic patients (Levy 2018). Based on prior experience with arbitrary time to antibiotic administration (see community acquired pneumonia), such draconian recommendations are likely to increase inappropriate use of antibiotics, distract clinicians from more important tasks and have minimal effect on patient outcomes. This is likely why the Infectious Disease Society of America (IDSA) declined endorsement of the SSC guidelines. The ridiculous nature of these recommendations has been discussed elsewhere.
Background: Despite minimal high-quality supporting evidence (Seymour 2017, Liu 2017, Ferrer 2014, Sterling 2015), regulatory bodies have pushed for benchmark times for administration of antibiotics in patients with sepsis. While most clinicians would agree that in patients with septic shock antibiotics should be given as quickly as possible, the same does not hold true for those patients with less severe infections. In the US, the Centers for Medicare and Medicaid Services (CMS) currently mandates that antibiotics be started in patients within 3 hours of onset of new organ dysfunction in patients with systemic inflammatory response syndrome and documented infection. The Surviving Sepsis Campaign (SSC) has even more extreme recommendations stating that antibiotics should be started within 1 hour from triage in septic patients (Levy 2018). Based on prior experience with arbitrary time to antibiotic administration (see community acquired pneumonia), such draconian recommendations are likely to increase inappropriate use of antibiotics, distract clinicians from more important tasks and have minimal effect on patient outcomes. This is likely why the Infectious Disease Society of America (IDSA) declined endorsement of the SSC guidelines. The ridiculous nature of these recommendations has been discussed elsewhere.
Even if the recommendation had some merit, it’s important to ask whether it’s even possible to implement. None of those on the SSC committee work in emergency departments and their understanding of the logistical challenges of such a policy is limited.
Article: Filbin MR et al. Antibiotic delays and feasibility of a 1-hour-from-triage antibiotic requirement: analysis of an emergency department sepsis quality improvement database. Ann Emerg Med 2019. PMID: 31561998
Clinical Question: Is a 1-hour-from-triage requirement for the administration of antibiotics in sepsis feasible?
Population: All adult ED patients (> 18 years) who met criteria for the current CMS Severe Sepsis and Septic Shock (SEP-1) definition – confirmed infectious source of high suspicion for infection and development of persistent hypotension (SBP < 90 mm Hg) on at least two measurements, or elevated lactate level > 4 mmol/L, or use of vasopressor medications in the ED.
Outcomes:
- Primary: Proportion of patients with delayed antibiotics administration (> 3 hours from documented onset of hypoperfusion and delay and > 1 hour from triage)
- Secondary: Time to antibiotics, rate of ICU admission and hospital mortality
Intervention: 12 months into the study period a sepsis care quality improvement intervention was initiated which involved a screening protocol (HR>SBP, SBP < 100 mm Hg, and clinical concern for infection). This study looks at delay to antibiotics before and after this intervention.
Design: Retrospective, cohort analysis from April 2014 to March 2016
Excluded: Patients receiving comfort measures only (unlikely to receive aggressive management), those transferred from an outside facility and already being treated for an infection.
Primary Results:
-
-
Total patients enrolled: 654
- Pre-intervention: 297
- Post-intervention: 357
- Patient characteristics were similar between the two cohorts
-
Total patients enrolled: 654
Critical Findings:
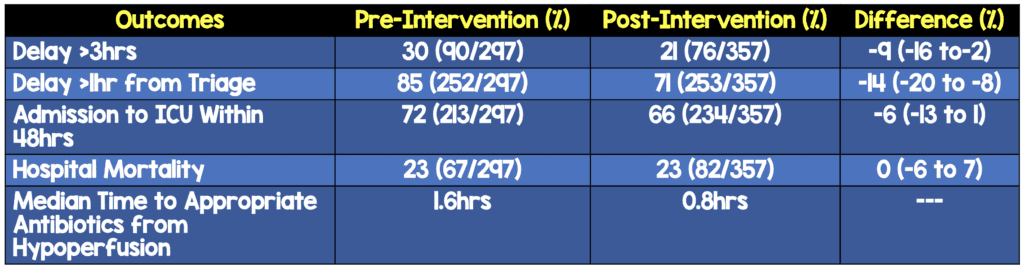
- No statistically significant difference between groups in terms of clinically meaningful outcomes
- 4 factors were independently associated with both definitions of antibiotic delay: Vague (non-explicitly infectious) presenting symptoms, triage location to nonacute areas, care before the quality improvement intervention, lower SOFA scores
Strengths:
- Asks an important clinical question that has not been addressed well to date
- Inclusion criteria were broad increasing the external validity of the findings
- Chart review methods are well detailed in the methods section
- Reviewers were blinded to encounter date and outcome
- Charts were reviewed by two reviewers independently and disagreements were resolved with a third reviewer
- Used the SPoT score for screening which has been shown to have better sensitivity than qSOFA score and similar specificity.
- Appropriate broad-spectrum antibiotics for sepsis were explicitly determined in accordance with CMS measures to ensure this was not a confounder in the outcome of mortality
- Baseline patient characteristics were generally similar between cohorts ensuring baseline balance in terms of comorbidities
Limitations:
- This was a single center study which decreases the external validity
- Retrospective review of charts which can only be as strong as the documentation in the charts
- Unclear the extent to which stress was placed on rapid antibiotic administration in the intervention training
- Diagnosis of sepsis based on billing codes which are subjective
- As with all before/after studies, the differences seen may have resulted from other trends independent of the intervention
- The study does not discuss the percent of patients who were misidentified as sepsis by the protocol and received unnecessary antibiotics
Discussion:
-
The intervention (only minimal details discussed in the manuscript) was able to produce a reduction in patients with delays in antibiotics. However, there are additional questions left unanswered:
- Attention is a zero-sum game. How did the extra attention to this set of patients affect delivery of care to other patients?
- How many patients ultimately not diagnosed with sepsis received unnecessary antibiotics? Were any of these patients harmed?
- More rapid administration of antibiotics is a surrogate outcome, not a patient centered one. Since the patient centered outcome (secondary – mortality) was not different between groups, the effort to reduce time to antibiotics is potentially wasted effort
- The pressure to rapidly administer antibiotics can lead to early diagnostic closure and hurt patients in the long-term.
- Metrics of ED crowding were not predictive of antibiotic delay, nor was difficult IV access, which suggests that timely antibiotic administration depended on diagnostic assessment, rather than operational factors
- Slightly more patients had hypotension at triage in the intervention arm (26.1% vs 18.9%) and the median active ED patient census at triage was higher during the intervention phase of the study (85 vs 73). This could mean that patients were potentially sicker during higher traffic times during the intervention arm compared to the pre-intervention arm
Authors Conclusions: “The quality improvement intervention significantly reduced antibiotic delays, yet most septic patients did not receive antibiotics within 1 hour of triage. Compliance with the 2018 Surviving Sepsis Campaign would require a wholesale alteration in the management of ED patients with either vague symptoms or absence of triage hypotension”
Our Conclusions: In this single-center study, implementation of sepsis protocols designed to expedite bundle delivery resulted in only a small fraction of patients receiving antibiotics within 1 hour of triage.
Potential to Impact Current Practice: This study validates the fact that administration of antibiotics in compliance with CMS measures (< 3 hours) is feasible while the administration of antibiotics within 1 hour of triage would require a complete overhaul of our current practices for all patients arriving with stable vital signs and/or vague nonspecific symptoms which could have a negative impact on patients not being evaluated for sepsis.
While this study will need external replication, it adds evidence regarding the feasibility (or lack thereof) of being able to deliver antibiotics within 1 hour of presentation for patients with sepsis.
Bottom Line: Despite education and institution of protocols, it may be logistically unrealistic to implement a 1-hour goal for administration of antibiotics to patients with sepsis. Before further efforts are made to meet this benchmark, real data proving benefit are necessary.
For More on This Topic Checkout:
- EM Nerd: The Case of the Hurried Objective
- PulmCrit: The Surviving Sepsis Campaign 1-Hour Bundle Is . . Back?
References:
- Seymour CW, Gesten F, Prescott HC, et al. Time to treatment and mortality during mandated emergency care for sepsis. N Engl J Med. 2017;376:2235-2244. PMID: 28528569
- Liu VX, Fielding-Singh V, Greene JD, et al. The timing of early antibiotics and hospital mortality in sepsis. Am J Respir Crit Care Med. 2017;196:856-863. PMID: 28345952
- Ferrer R, Martin-Loeches I, Phillips G, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Crit Care Med. 2014;42:1749-1755. PMID: 24717459
- Sterling SA, Miller WR, Pryor J, et al. The impact of timing of antibiotics on outcomes in severe sepsis and septic shock: a systematic review and meta-analysis. Crit Care Med. 2015;43:1907-1915. PMID: 26121073
- Levy MM, Evans LE, Rhodes A. The Surviving Sepsis Campaign bundle: 2018 update. Intensive Care Med. 2018;44:925-928. PMID: 29767636
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post Are Antibiotics for Sepsis in One Hour Feasible in the ED? appeared first on REBEL EM - Emergency Medicine Blog.