
 Background: Use of contrast media in CT scans has been cited as one of the most common causes of iatrogenic acute kidney injury. Its use however improves the diagnostic accuracy of CT scans. Some studies have even reported an incidence of contrast induced nephropathy (CIN) as high as 14%. Many of the studies coming to these conclusions were performed before the use of low- and iso-osmolar contrast agents. Also to date, all controlled studies on this topic have been observational and not randomized controlled trials. More recent propensity-scored analyses have had conflicting results. One study found no increased risk of acute kidney injury, dialysis or mortality regardless of baseline renal function, while others have found increased acute kidney injury in patients with renal dysfunction. This current study tried to clarify the incidence of acute kidney injury attributable to IV contrast media administration.
Background: Use of contrast media in CT scans has been cited as one of the most common causes of iatrogenic acute kidney injury. Its use however improves the diagnostic accuracy of CT scans. Some studies have even reported an incidence of contrast induced nephropathy (CIN) as high as 14%. Many of the studies coming to these conclusions were performed before the use of low- and iso-osmolar contrast agents. Also to date, all controlled studies on this topic have been observational and not randomized controlled trials. More recent propensity-scored analyses have had conflicting results. One study found no increased risk of acute kidney injury, dialysis or mortality regardless of baseline renal function, while others have found increased acute kidney injury in patients with renal dysfunction. This current study tried to clarify the incidence of acute kidney injury attributable to IV contrast media administration.
What They Did:
- Single center retrospective cohort analysis of >17,000 patients who underwent contrast enhanced, non-contrast enhanced, or no CT
- Intervention: CT scan with or without intravenous contrast
Outcomes:
- Primary: Incidence of acute kidney injury
- Absolute increase in serum creatinine level ≥0.5mg/dL or ≥25% increase over baseline serum creatinine level at 48 – 72 hours after imaging
- Acute Kidney Injury Network/Kidney Disease Improving Global Outcomes (AKIN/KDIGO) Guidelines
- Stage 1: Absolute increase in serum creatinine level ≥0.3mg/dL or a 1.5 – 1.9 fold increase over baseline serum creatinine level
- Stage 2: 2.0 – 2.9 fold increase over baseline serum creatinine level
- Stage 3: 3 fold increase over baseline serum creatinine level
- Increase to serum creatinine level ≥4.0 mg/dL
- Initiation of Dialysis
- Secondary: New chronic kidney disease, dialysis, and renal transplantation at 6 months
Inclusion:
- Age ≥18 years
- Received a CT with or without contrast enhancement in the ED
- Initial serum creatinine level measured 8 hours before CT and 48 – 72 hours after CT
Exclusion:
- Initial serum creatinine <0.4 mg/dL (to minimize inclusion of random lab error as cases of acute kidney injury)
- Serum creatinine level ≥4.0 mg/dL (already meeting partial criteria for severe acute kidney injury)
- Insufficient serum creatinine level data
- History of renal transplant
- Ongoing or previous dialysis
- ED visit in the 6 months before the study start date
- CT scan performed in the 6 months preceding the index ED visit
- Contrast-enhanced CT performed within 72 hours of ED departure
Results:
- 17,934 patient visits from 16,801 unique patients included in final analysis
- Factors most strongly associated with increased probability of acute kidney injury were:
- Increased age
- Administration of nephrotoxic medications
- Preexisting diagnosis of CHF or CKD
- Hypoalbuminemia
Strengths:
- Large study that was powered to detect a difference in incidence of acute kidney injury as low as 1.5%
- Largest controlled study of acute kidney injury after contrast media administration in the ED
- Used multiple definitions of acute kidney injury to ensure primary outcome not under reported
- Reduced selection bias by using propensity-score matching to estimate the effect of contrast media on acute kidney injury
- Inclusion of 2 control populations (i.e. non-enhanced & no CT) strengthens the findings of the study
Limitations:
- Single Center Study
- Majority of patients studied admitted to hospital, meaning they were more ill, and could potentially be at higher risk for developing acute kidney injury versus patients discharged home
- Retrospective observational study limited examination of comorbidities and outcomes to those recorded in the institutional electronic medical record
- This analysis did not capture nephroprotective or nephrotoxic interventions performed after patients departed the ED
- Although the authors attempted to minimize bias associated with treatment assignment by using propensity score matching, there still may be some factors that were not included and could affect results of this study
Discussion:
- It is possible that nephroprotective practice patterns may be partially responsible for the observations in this study:
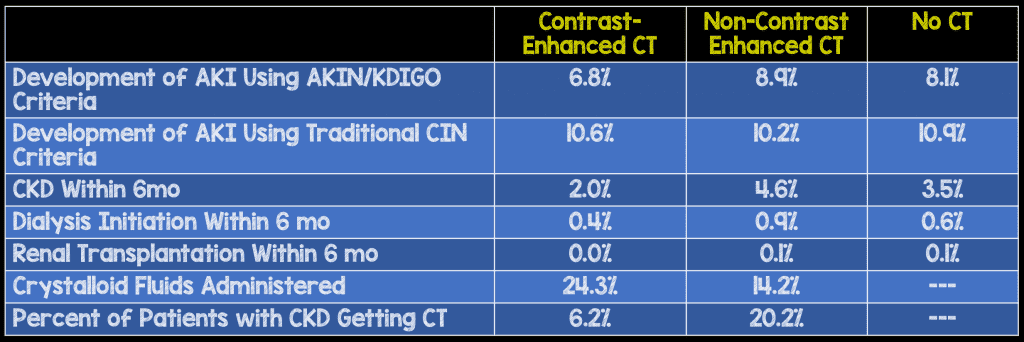
- Clinicians less likely to administer contrast media to patients with decreased baseline renal function (6.2% vs 20.2%)
- Clinicians more likely to administer intravenous fluids prior to enhanced CT scans vs non-enhanced CT scans (24.3% vs 14.2%)
Author Conclusion: “In the largest well-controlled study of acute kidney injury following contrast administration in the ED to date, intravenous contrast was not associated with an increased frequency of acute kidney injury.”
Clinical Take Home Point: It is time for a controlled randomized prospective trial to determine if the newer hypo- and iso-osmolar intravenous contrast media lead to the development of acute kidney injury or not.
References:
- Hinson JS et al. Risk of Acute Kidney Injury After Intravenous Contrast Media Administration. Ann Emerg Med 2017; S0196 – 0644(16): 31388 -9. PMID: 28131489
For More Thoughts on This Topic Checkout:
- Ryan Radecki at Emergency Literature of Note: Punching Holes in CIN
- Josh Farkas at PulmCrit(EMCrit): Do CT Scans Cause Contrast Nephropathy?
- Richard Sinert on EMDocs: Contrast-Induced Nephropathy – Confounding Causation
- Jeremy Faust & Lauren Westafer on FOAMcast: Contrast-Induced Nephropathy and Genitourinary Trauma
- Joel Topf at Precious Bodily Fluids Blog: Confirmation Bias, Cognitive Dissonance, and Contrast Nephropathy
Post Peer Reviewed By: Anand Swaminathan (Twitter: @EMSwami)
The post Contrast Induced Nephropathy (CIN): Fact or Myth? appeared first on REBEL EM - Emergency Medicine Blog.