
 Background: In cardiac arrest, high quality, uninterrupted CPR is essential to help improve survival rates. In theory, mechanical CPR should provide CPR at a standard depth and rate for prolonged periods without a decline in quality, which should help improve survival and survival with good neurologic outcomes. There are many types of mechanical chest compression devices but the two main technologies can be generalized as piston devices and load-distributing bands. The piston driven devices work by compressing on the chest in an up and down type of motion, similar to how we do manual CPR. The load distributing bands wrap all the way around the chest and shorten and lengthen which provides more of a rhythmic type of chest compression. No individual trials have ever shown superiority on clinically important outcomes for adult patients with OHCA, regardless of device.
Background: In cardiac arrest, high quality, uninterrupted CPR is essential to help improve survival rates. In theory, mechanical CPR should provide CPR at a standard depth and rate for prolonged periods without a decline in quality, which should help improve survival and survival with good neurologic outcomes. There are many types of mechanical chest compression devices but the two main technologies can be generalized as piston devices and load-distributing bands. The piston driven devices work by compressing on the chest in an up and down type of motion, similar to how we do manual CPR. The load distributing bands wrap all the way around the chest and shorten and lengthen which provides more of a rhythmic type of chest compression. No individual trials have ever shown superiority on clinically important outcomes for adult patients with OHCA, regardless of device.
What Article are we Discussing?
- Gates S et al. Mechanical Chest Compression for Out of Hospital Cardiac Arrest: Systematic Review and Meta-Analysis. Resuscitation 2015; 94: 91 – 97. PMID: 26190673
What They Did:
- Systematic review of studies evaluating effectiveness of mechanical chest compressions vs manual chest compressions in adult patients with Out of Hospital Cardiac Arrest (OHCA)
- Good Neurologic Outcome defined as Cerebral Performance Category (CPC) ≤2 or Modified Rankin Scale (mRS) Score ≤3
Outcomes:
- Return of Spontaneous Circulation (ROSC)
- Survival of Event
- Overall Survival
- Survival with Good Neurologic Outcome
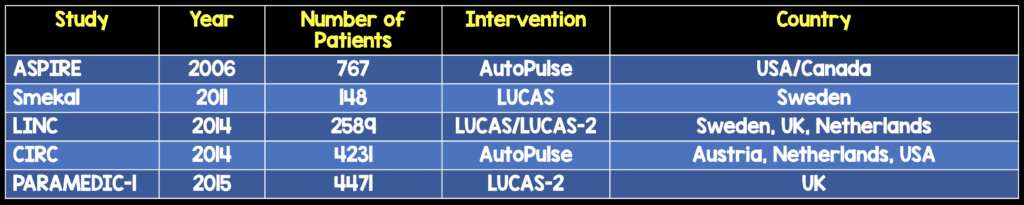
Trials Included:
Results:
- 5 Trials included
- 3 Evaluated LUCAS or LUCAS-2 Devices
- 2 Evaluated Autopulse Device
- No Advantage of Mechanical Chest Compression Devices for:
- ROSC (OR 0.96)
- Survival of Event (OR 0.95)
- Survival to Discharge or at 30 days (OR 0.89)
- Survival with Good Neurological Outcomes (OR 0.76)
Strengths:
- Used Cochrane Risk of Bias tool to assess studies’ risk of bias
- Very low proportion of missing outcome data (But in some trials missing data in the assessment of neurologically intact survival was missing, which could cause potential bias)
Limitations:
- No blinding of clinicians providing care
Discussion:
- This review looked at 5 randomized trials, with over 10,000 patients with OHCA and found no evidence of benefit with the use of mechanical chest compression devices, but lets be clear, it also found no evidence of harm.
- There are very wide confidence intervals despite the large number of patients, and this is most likely due to the low survival rate from OHCA
- Quality of CPR provided in the manual CPR arms was not documented in studies. This is an important point that cannot be emphasized enough. If manual CPR was high quality, then maybe mechanical devices may not seem as good, but if the CPR was low quality, then mechanical devices may be better.
- Another issue is in the 2006 ASPIRE trial mechanical CPR was at a rate of 80 compressions/min and manual CPR was at 100 compressions/min. This would falsely lower the usefulness of mechanical CPR as we know the appropriate compression rate is 100/min.
- Another issue is that in the 2006 ASPIRE study, time to defibrillation was 2.1 minutes longer than the manual CPR arm. In the LINC trial, time to defibrillation was 1.5 minutes longer than the manual arm. We know that early, high-quality CPR + early defibrillation are keys to successful survival with good neurologic outcome.
- CPR is a means to an end. In other words doing high quality, uninterrupted CPR is important, but this is not the end point. Instead this is a way to continue to perfuse the brain while we figure out what caused the OHCA. Therefore, mechanical CPR is a way to cognitively offload our minds about depth of compressions, rate of compressions, while we try and figure out why our patient arrested.
- Mechanical CPR still has a role in my opinion. Imagine working in an ED where you are the lone doctor with minimal staff. You only have so many people that can perform CPR before they get tired and the quality of the CPR decreases. Imagine another scenario like being on the back of an ambulance or a helicopter as a patient is being transported. Surely, mechanical CPR will be higher quality and safer for the crew than manual CPR? I would consider using mechanical CPR over manual CPR in the following scenarios:
- Limited rescuers available
- Prolonged CPR
- CPR in a moving ambulance or helicopter
Author Conclusion: Existing studies do not suggest that mechanical chest compression devices are superior to manual chest compression, when used during resuscitation after OHCA
Clinical Take Home Point: This is not the end of mechanical compression devices as none of the studies showed harm with these devices. Use of these devices may cognitively offload providers to focus on the cause of the arrest instead of ensuring the quality of the CPR.
References:
- Gates S et al. Mechanical Chest Compression for Out of Hospital Cardiac Arrest: Systematic Review and Meta-Analysis. Resuscitation 2015; 94: 91 – 97. PMID: 26190673
For More Thoughts on This Topic Checkout:
- Salim Rezaie at ALiEM: Mechanical vs Manual CPR Chest Compressions
- Sean Kivlehan at ALiEM: Mechanical CPR and the LINC Trial
- Simon Carley at St. Emlyn’s Blog: JC – PARAMEDIC Trial m-CPR at St.Emlyn’s
- Cliff Reid at Resus.Me: Not Finding A Difference Doesn’t Prove Equivalence
- Rory Spiegel at EMLit of Note: Man vs Machine – A CPR Battle to the…
- Ryan Radecki at EMLit of Note: CPR – Crushing it With Machines
- Ryan Radecki at EMLit of Note: More Futility for Mechanical CPR
- Ken Milne at The SGEM: SGEM#136 – CPR – Man or Machine
- The Resus Room: Mechanical CPR
Post Peer Reviewed By: Matt Astin (Twitter: mastinmd)
The post CPR in Out of Hospital Cardiac Arrest: Man vs Machine appeared first on REBEL EM - Emergency Medicine Blog.