
 Background: The two biggest keys to successful survival with good neurological outcome in out-of-hospital cardiac arrest (OHCA) are high-quality CPR and early defibrillation. Dispatcher-assisted (DA) CPR is a novel concept to not only improve the rate of CPR being performed, but also the quality of CPR. In DA-CPR, rescuers perform CPR under telephone guidance from trained dispatchers. In this study, the authors sought to see if DA-CPR improved the quality of chest compressions (Compression depth, compression rate, no-flow time, complete release of pressure between compressions, and hand location).
Background: The two biggest keys to successful survival with good neurological outcome in out-of-hospital cardiac arrest (OHCA) are high-quality CPR and early defibrillation. Dispatcher-assisted (DA) CPR is a novel concept to not only improve the rate of CPR being performed, but also the quality of CPR. In DA-CPR, rescuers perform CPR under telephone guidance from trained dispatchers. In this study, the authors sought to see if DA-CPR improved the quality of chest compressions (Compression depth, compression rate, no-flow time, complete release of pressure between compressions, and hand location).
What They Did:
- Parallel, randomized controlled, open label trial
- Evaluate the efficacy of DA in improving CPR quality among healthcare professionals and laypersons within a multi-ethnic Southeast Asian population during a simulated cardiac arrest
- Participants randomized to CPR with DA over the phone (DA+) vs CPR without DA (DA-)
Outcomes:
- Primary: CPR compression depth, compression rate, no-flow time, complete release of pressure between compressions, and hand location
- Secondary: Identify which subgroups benefit from DA and if improved, which parameters of CPR quality improve
Inclusion:
- General public and healthcare workers (doctors, nurses, dentists, allied health professionals, medical students, nursing students, dental students, emergency medical technicians, and CPR instructors)
- Ages 21 – 70 years
- English speaking
Exclusion:
- Physical or communication disabilities precluding CPR performance
Results:
- 412 participants recruited
- No difference in other primary outcomes (compression depth, no-flow time, complete release between compressions, or hand location)
- Healthcare professionals in DA+ had a higher proportion of correct hand location compared to those in DA- (82.1% vs 53.3%)
- NO difference in CPR quality among laypersons with valid CPR certification regardless of whether they received DA
Strengths:
- 1strandomized control trial to assess impact of DA on CPR quality in both healthcare professionals and laypersons
- Patients randomized by study team member, who was not involved in participant recruitment
- Used 3 independent assessors to reduce observer bias and to ensure reliability and validity of visual analysis of CPR
- Zero participants lost to follow up and only 4 participants excluded from the analysis
- No difference in baseline characteristics of participants between groups with the exception of more healthcare professionals in the DA+ cohort vs DA- cohort (13.7% vs 21.1%; p = 0.050), however this was accounted for using a stratified analysis
- Mannequins assessed quality of chest compressions including compression depth, and compression rate
Limitations:
- Used convenience sampling instead of consecutive sampling, which could have recruited participants that were more interested and competent in performing CPR compared to the general public
- Valid CPR certification was considered to be valid if participant had received CPR training within the past two years.
- Once the intervention began, neither participants nor assessors were blinded which could influence results of the study
- Simulation was only carried out for 2 minutes, which is a short CPR time, and may not be as generalizable to longer resuscitations
- Hand location was considered to be correct if the participant maintained correct hand location for ≥50% of the time. This means that 49% of the time the hands may have been in the incorrect position, which is not adequate CPR
- Small sample size of participants that were non-healthcare with CPR certification precludes a clear conclusion on the effectiveness of DA among this group
- Performed at a single location at a hospital’s common area which may over-represent healthcare professionals and reduce the external validity of the findings
Discussion:
- Dispatcher used a very specific script:
- I need you to place your right hand on the centre of his/her chest, between the nipples.
- If the rescuer asks which part of the hand to use, tell him/her to place the whole palm on the chest.
- Place your left hand on top of your right hand and interlock your fingers.
- Make sure your elbows are straight.
- Now, I need you to do chest compressions to a depth of 5cm.
- If rescuer asks how he/she will know he/she is at 5cm, tell him/her to just push hard and push fast. It is okay if he/she breaks the ribs.
- You will need to push hard and push fast at a rate of 100 per min. Count together with me. We will do it in sets of 10. Are you ready?
- Okay, 1… 2… 3… (count in sets of 10 for the 2-minute period).
- Have the paramedics arrived yet? I am going to let you go. The paramedics will take over.
Author Conclusion: “DA should be provided to laypersons without valid CPR certification, as well as healthcare professionals. The identification of gaps in the current DA protocol highlights areas where specific changes can be made to improve CPR quality.”
Clinical Take Home Point: To be fair this is not the world’s best study, but I do think there are a few take away points that require emphasis:
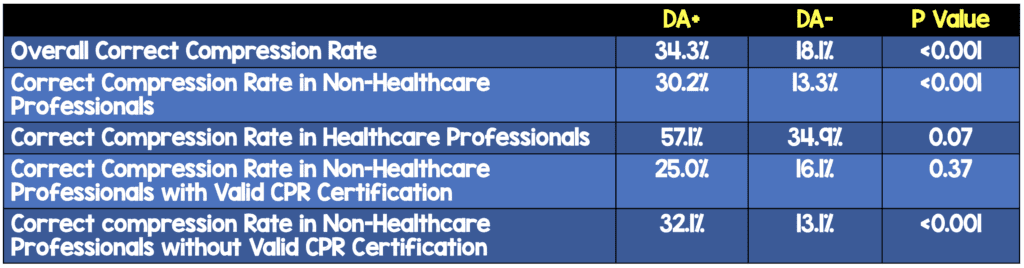
- CPR quality in health professionals was poor with an appropriate compression rate being achieved 34.9% – 57.1% of the time and appropriate compression depth being achieved 35.7% – 48.8%.We need to do better as healthcare professionals.
- In this small single-center study DA-CPR appears to improve compression rates in non-healthcare, non-CPR certified laypersons (32.1% vs 13.1%) with a NNT = 5, BUT did not appear to improve compression depth, no-flow time, or complete releases during CPR in any of the other cohorts.
References:
- Nelson TMH et al. The Use of Dispatcher Assistance in Improving the Quality of Cardiopulmonary Resuscitation: A Randomised Controlled Trial. Resus 2019. PMID: 30876922
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)
The post Dispatcher-Assisted Cardiopulmonary Resuscitation (DA-CPR) appeared first on REBEL EM - Emergency Medicine Blog.