
 Background: Serial lactate measurements is a common core measure that we follow in septic shock resuscitation. A number of readers have written in enquiring about whether resuscitation with lactated ringers instead of 0.9% saline would lead to increases in serum lactate. It’s a great question, and one that I am not sure I had a solid answer for before reviewing this topic. LR contains 28 mmol/L of sodium lactate and, on the surface, it seems reasonable to think that infusion of LR would lead to lactate increases. This could potentially confound the interpretation of serial serum lactate measurements.
Background: Serial lactate measurements is a common core measure that we follow in septic shock resuscitation. A number of readers have written in enquiring about whether resuscitation with lactated ringers instead of 0.9% saline would lead to increases in serum lactate. It’s a great question, and one that I am not sure I had a solid answer for before reviewing this topic. LR contains 28 mmol/L of sodium lactate and, on the surface, it seems reasonable to think that infusion of LR would lead to lactate increases. This could potentially confound the interpretation of serial serum lactate measurements.
What They Did:
- Double-blind randomized controlled trial
- 30 healthy volunteers assigned to receive 30cc/kg of either LR or 0.9% saline (NS)
- Serum lactate measured before and after fluid bolus
Outcomes:
- Primary: Difference in change in serum lactate levels between LR and NS groups
- Secondary:
- Change in pH
- Change in bicarbonate
- Change in sodium
- Change in chloride
- Change in creatinine
Inclusion:
- Healthy volunteers (i.e. No acute symptoms and met none of the exclusion criteria)
- Aged ≥18 years of age
Exclusion:
- Pregnant
- Breastfeeding
- Prisoners
- History of conditions associated with fluid overload (CHF, renal, or hepatic failure)
- Baseline serum lactate level >2.2 mmol/L
- Baseline creatinine >1.5 mg/dL
Results:
- 30 patients randomized with 15 patients in each arm
- Fluid bolus given with a pressure bag through a peripheral 18g IV. On average the bolus took 47 minutes
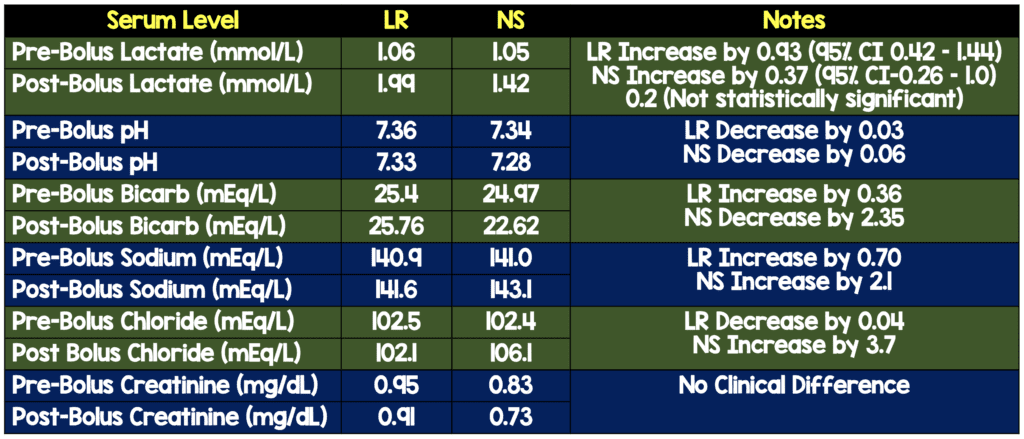
- Changes seen above are consistent with hyperchloremic metabolic acidosis in the NS group
Strengths:
- Randomized, double-blind, controlled trial
- Pharmacist with no role in data collection prepared fluids using an opaque black bag to obscure the fluids
- Fluid volume given is similar to what we would see in septic patients
- Baseline characteristics of the groups were similar
Limitations:
- These were healthy volunteers, not septic patients, or patients with other comorbid conditions. These results can’t be translated to actual patients
- Small cohort of patients.
- Serum lactate levels were drawn 5 minutes after the conclusion of the IV fluid administration, would have been nice to see longer periods of time (i.e. 30, 60, 90, 120 minutes) to see rates of change and duration of effects
- Primary outcome was a lab-oriented outcome, not a patient oriented outcome
Discussion:
- There was another RCT published in Crit Care Med 1997 [2] trying to answer this question as well. 24 healthy, adult volunteers received 1hr infusions of LR (n = 6), NS (n = 6), dextrose in LR (n = 6), or D5W (n = 6). The study evaluated LR vs NS and showed no difference in lactate levels in patients. The study was limited by the fact that patients only received 1L of LR or NS over 1hr, which is not the current 30cc/kg fluid bolus we currently give septic patients.
- Study powered to detect a 0.5mmol/L mean change in lactate levels, which is a reasonable value.Important to realize this value was chosen by clinical gestalt based on what the authors considered to be clinically significant (i.e. an arbitrary value in my opinion).
- Both groups had 1 outlier lactate level >5mmol/L corresponding with the second and third subjects enrolled in the study. After these two patients, all lactate levels >2mmol/L were confirmed with repeat levels. The authors appropriately removed these two patients and re-analyzed the data to find a statistically significant between group difference in serum lactate level of 0.65mmol/L. Outlier levels would therefore have a huge impact on results
- Although not statistically significant 14 out of 15 patients in the LR group did have an elevated serum lactate with 6 of them having a lactate level >2mmol/L. Only 7 out of 15 patients in the NS groups had increases in lactate, with only 2 of them having lactate levels >2mmol/L
- One important caveat is that there are many resuscitation medications that may not be compatible with LR (piperacillin-tazobactam, TXA, blood products, etc…) and in these cases, a second IV line with NS is what I typically use in the cases that these medications are needed.
- Lactate is known to be cleared by the liver and kidney, so it is unclear what this effect would be in patients with hepatic and renal dysfunction, as this was a healthy patient population, but the lactate levels will most likely be higher than the values shown in this study
Author Conclusion: “In healthy individuals, a modest but significant rise in mean serum lactate was seen after a 30cc/kg LR bolus. There was no difference in mean serum lactated when comparing a 30mL/kg bolus of NS to LR.”
Clinical Take Home Point: In healthy volunteers the use of 30cc/kg of LR or NS both slightly increase lactate levels, however the duration of this effect, effect on patient oriented outcomes, effect on patients with renal/liver impairment, and the effect on patients with acute illness cannot be generalized based on this study. I will continue to use balanced crystalloids in large volume resuscitations until further evidence indicates that this is causing harm to patients.
References:
- Zitek, T et al. Does Intravenous Lactated Ringer’s Solution Raise Serum Lactate? JEM 2018. PMID: 30037514
- Didwania A et al. Effect of Intravenous Lactated Ringer’s Solution Infusion on the Circulating Lactate Concentration: Part 3. Results of a Prospective, Randomized, Double-Blind, Placebo-Controlled Trial. Crit Care Med 1997. PMID: 9366769
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)

The post Does Lactated Ringers (LR) Raise Serum Lactate? appeared first on REBEL EM - Emergency Medicine Blog.