
 There are approximately 8 to 10 million patients complaining of chest pain coming to Emergency Departments (EDs) in the United States annually. In the US, we use a very liberal testing strategy in order to avoid acute coronary syndrome (ACS) in patients presenting with chest pain. This results in over 50% of ED patients with acute chest pain receiving serial cardiac biomarkers, stress testing, and cardiac angiography at an estimated cost of $10 to $13 billion annually and yet fewer than 10% of these patients are diagnosed with ACS.
There are approximately 8 to 10 million patients complaining of chest pain coming to Emergency Departments (EDs) in the United States annually. In the US, we use a very liberal testing strategy in order to avoid acute coronary syndrome (ACS) in patients presenting with chest pain. This results in over 50% of ED patients with acute chest pain receiving serial cardiac biomarkers, stress testing, and cardiac angiography at an estimated cost of $10 to $13 billion annually and yet fewer than 10% of these patients are diagnosed with ACS.
Despite these numbers the American College of Cardiology/American Heart Association (ACC/AHA) recommends that low-risk chest pain patients receive serial cardiac markers followed by some sort of provocative/objective cardiac testing. Using this strategy amongst low-risk chest pain patients unnecessarily uses resources on those least likely to benefit. Low-risk chest pain patients have ACS rates of <2% and provocative/objective cardiac testing is associated with a significant amount of “downstream” testing (i.e. cardiac catheterization) due to false positive tests.
To date, the HEART score has been examined in >6000 patients and demonstrated a high NPV for MACE at 6 weeks exceeding 98%, but until now there has been no randomized trial.
What is the HEART Pathway?
The HEART Pathway is a combination of the HEART score with 0 and 3 hour cardiac troponin testing. This is a recently developed decision aid used to identify patients in the emergency department (ED) that are safe for early discharge. There have been several observational studies that have shown using the HEART score can classify >20% of patients with acute chest pain for early discharge while maintaining a negative predictive value (NPV) for major adverse cardiac events (MACE) rate of >99% at 30 days. There have been no real-time, randomized trials comparing the HEART Pathway versus the ACC/AHA recommendations (i.e. usual care), until now.
How was the HEART Pathway Applied?
Patients were recruited from a tertiary care academic medical center in North Carolina which has a patient volume of >100,000 patients/year. This was a randomized, controlled, single-center study which was funded by the AHA that sought to compare the HEART Pathway versus usual care to see if the HEART Pathway could reduce objective cardiac testing, increase early discharges, reduce index hospital length of stay while maintaining a high sensitivity and NPV (>99%) for MACE.
Patients were randomized to the HEART Pathway or usual care arms. In the HEART Pathway arm, patients were risk stratified by attending ED providers using the HEART score and serial troponin measures at 0 and 3 hours after ED presentation. A HEART score of 0 – 3 was classified as a low-risk assessment, whereas a score of ≥4 was classified as a high-risk assessment. Usual care was at the discretion of the ED, but providers were encouraged to follow the ACC/AHA guidelines, which recommended serial cardiac biomarkers and objective/provocative cardiac testing before discharge from the observation unit or inpatient ward for patients with symptoms suggestive of ACS. The HEART Pathway algorithm is shown in the figure below.
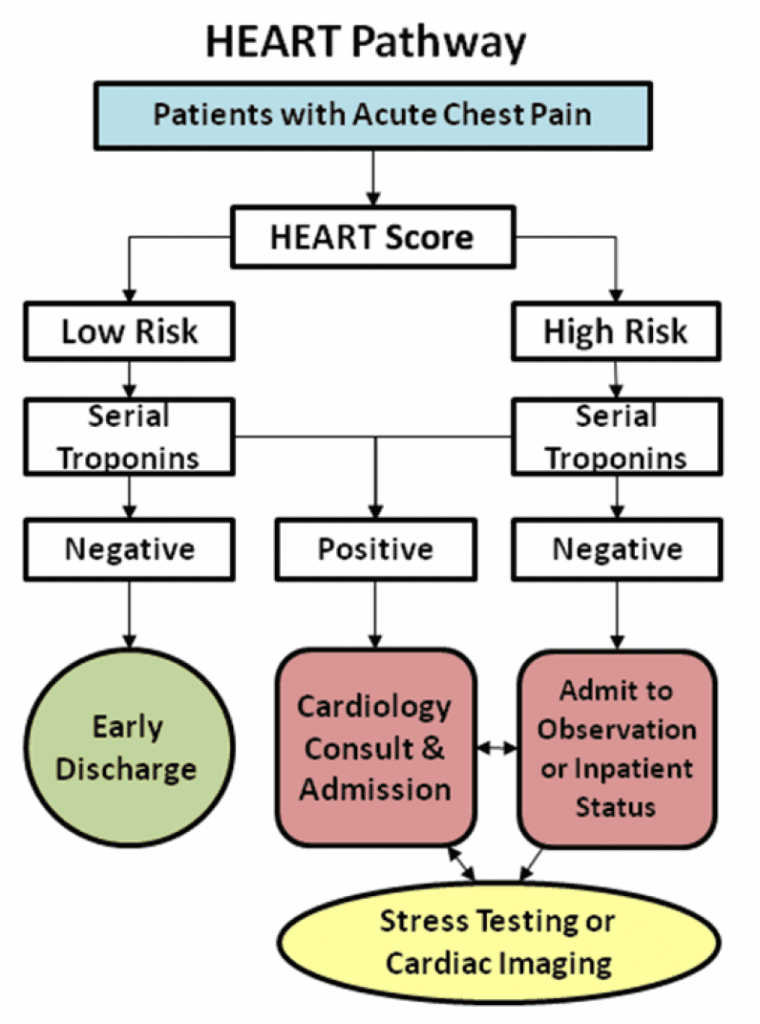
Image from Mahler SA et al. The HEART Pathway Randomized Trial Identifying Emergency Department Patients With Acute Chest Pain for Early Discharge. Circ Cardiovasc Qual Outcomes March 2015; 8 (2): 195 – 203.
What Were the Outcomes Assessed?
- Primary Outcome: Rate of objective cardiac testing within a 30 day period from presentation defined as stress testing, coronary computed tomographic angiography (CCTA), or invasive coronary angiography.
- Secondary Outcome: Discharge rate*, index length of stay (LOS), cardiac related recurrent ED visits and non-index hospitalization at 30 days.
- Safety Outcome: Composite of MACE (Included all cause mortality, myocardial infarction, or coronary revascularization) within 30 day follow up from index visit
*Early discharge is defined as discharge from the ED without objective cardiac testing
What Were the Results of this Study?
- A total of 282 patients with 141 patients in each arm of the study
- Use of the HEART Pathway resulted in identification of 46.8% of patients as low risk
- Objective Cardiac Testing: HEART Pathway 56.7% vs Usual Care 68.8% (Absolute testing reduction of 12.1%)
- Early Discharge Rate: HEART Pathway 39.7% vs Usual Care 18.4% (Absolute early discharge increase of 21.3%)
- Median LOS: HEART Pathway 9.9 hrs vs Usual Care 21.9 hrs (Absolute median reduction in LOS of 12 hrs)
- Zero patients identified as low risk by HEART Pathway had an index or non-index MACE
What Were the Strengths of this Study?
- No participants were removed from the study after randomization
- 30 day follow up rate was 96% and of the 10 patients lost to follow up, non appeared in the Social Security Death master file
- MACE rate of 5.7% in HEART Pathway arm and 6.4% in the usual care arm, which is higher than the 2 – 3% MACE rate seen in the accelerated diagnostic protocol and CCTA studies
What Were the Limitations of this Study?
- The sample size of 282 patients was small and recruitment from a single academic center may limit generalizability to community settings
- This study was not powered to detect differences in MACE
- The inter-observer agreement of low vs high risk patients by HEART score was only moderate with a kappa of 0.63
- Non-adherence to the HEART Pathway occurred in 29% (19/66) of low-risk patients and 13% of high risk patients. Perfect adherence among high and low risk patients would have increased early d/c rate to 46.8%. Although this is a high rate of non-adherence this is not so different from other studies evaluating clinical decision aids and by allowing non-adherence, this study may provide a more accurate determination of “real world” practice.
What is the Clinical Take Home Message of this Study?
It is safe to begin using the HEART Pathway (Non-ischemic ECG, HEART Score, and Troponin testing at 0 and 3 hours) in chest pain patients presenting to the emergency department with suspicion of ACS. Use of the HEART Pathway significantly decreases objective cardiac testing, increases early discharge rates, and cuts median length of stay with a zero MACE rate at 30 days (Study not powered for MACE).
References:
- Mahler SA et al. The HEART Pathway Randomized Trial Identifying Emergency Department Patients With Acute Chest Pain for Early Discharge. Circ Cardiovasc Qual Outcomes March 2015; 8 (2): 195 – 203. PMID: 25737484
Post Peer Reviewed By: Anand Swaminathan (Twitter: @EMSwami)
For More on the Above Topic Checkout:
- Amal Mattu at EMCast
- Ken Milne at The SGEM: SGEM #151 – Groove is the HEART Pathway
- Ben Short at The Bottom Line: Mahler
The post Is it Time to Start Using the HEART Pathway in the Emergency Department? appeared first on REBEL EM - Emergency Medicine Blog.