
 Traditionally, vasopressor infusions have been done through central venous catheters (CVCs) due to the hypothetical risk of extravasation injury to extremities when given through peripheral IVs. The documented risk of extravasation from peripheral pressors is 3 – 6% [1][3][4][5]. Hypothetically, the extravasation rate can be further reduced. At Essentials of EM 2020 I gave a short 10-minute talk on 6 pearls I have implemented. This post will serve as a summary of that talk.
Traditionally, vasopressor infusions have been done through central venous catheters (CVCs) due to the hypothetical risk of extravasation injury to extremities when given through peripheral IVs. The documented risk of extravasation from peripheral pressors is 3 – 6% [1][3][4][5]. Hypothetically, the extravasation rate can be further reduced. At Essentials of EM 2020 I gave a short 10-minute talk on 6 pearls I have implemented. This post will serve as a summary of that talk.
Pearl #1: Use Proximal Veins
- Use veins in the antecubital fossa or more proximal
- These are larger veins which allow for larger IVs and decrease the chances of puncturing the back wall of the vein
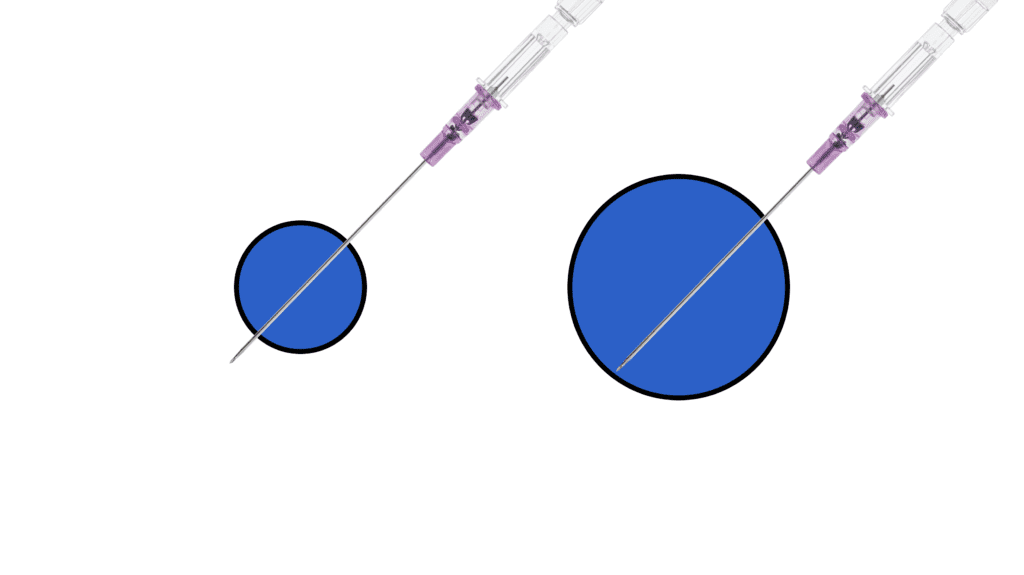
- Go with the biggest most superficial vein so that we don’t conceal extravasation in deeper veins
- Not all of these IVs will be US-guided, but for deeper veins will need to use sterile technique with a linear probe
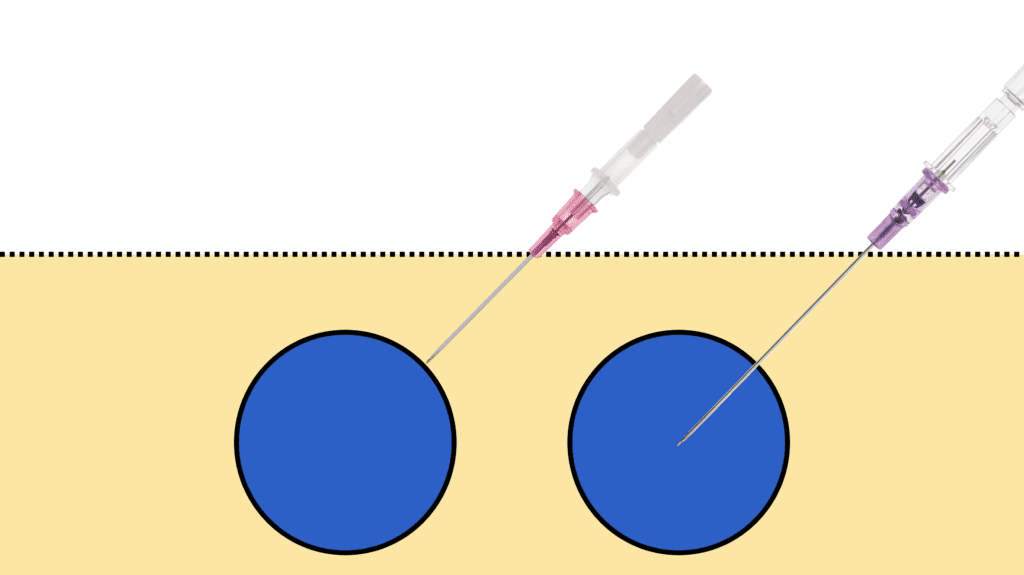
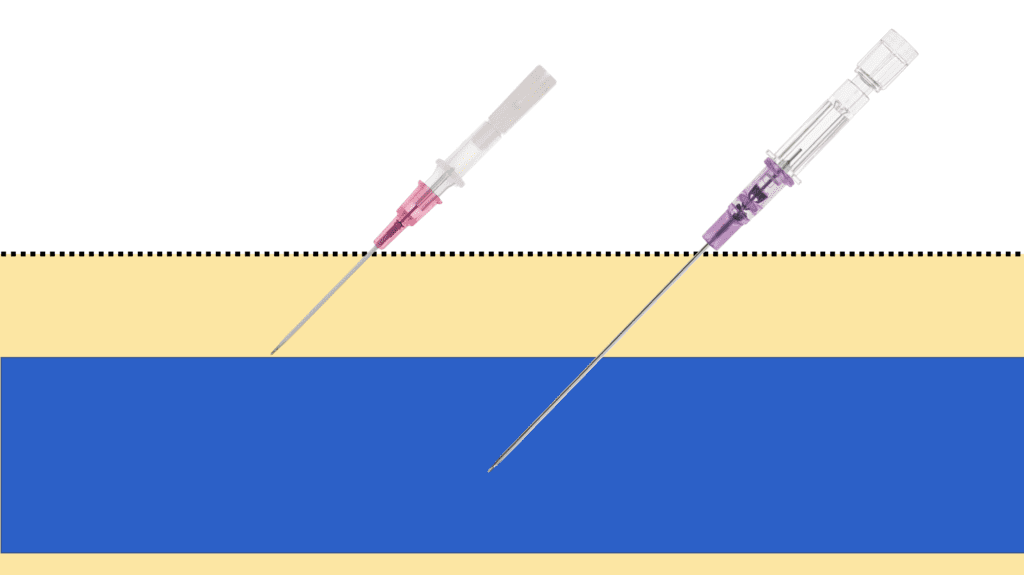
Pearl #2: Use an Ultralong Catheter
- IV catheters come in varying lengths, including:
- Standard: 2.95cm (1.16in)
- Long: 4.78cm (1.88in)
- Ultralong: 6.35cm (2.5in)
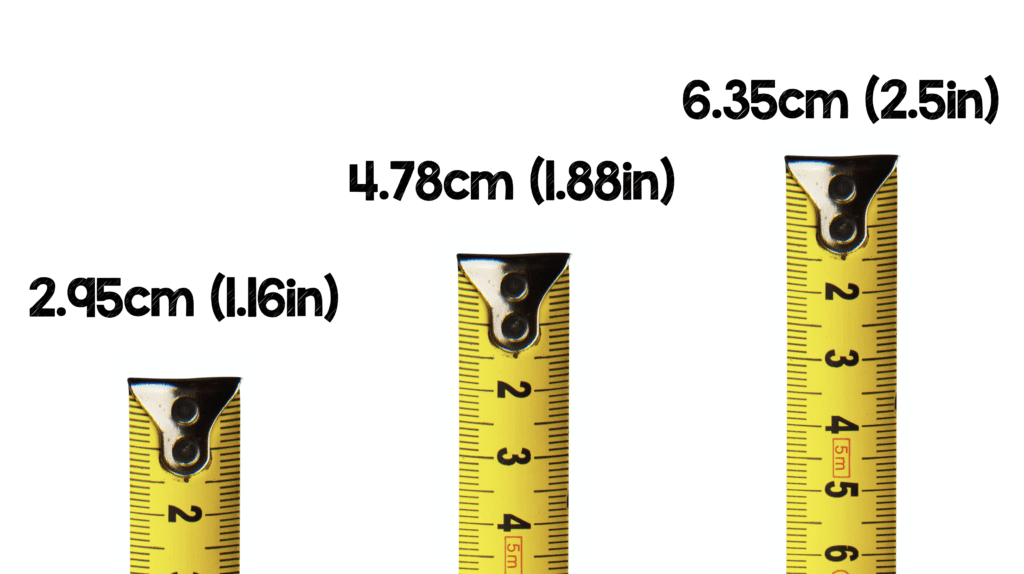
- If we are using more proximal veins, then we have more subq tissue to traverse. Therefore, we want to ensure the catheter we use is able to get >2.75cm into the vein [3] to avoid the catheter coming out. In some cases a long catheter (4.78cm) may be more than enough
Pearl #3: Limit the Time of Infusion
- Peripheral vasopressors should be considered a bridge to somewhere…
- The patient improves, in which case you can stop the infusion
- The patient doesn’t improve in which case you should insert a midline or CVC
- The longer you run this infusion, the more chance of extravasation. According to my interpretation of the literature, the longest we should be running these infusions peripherally is 4hrs
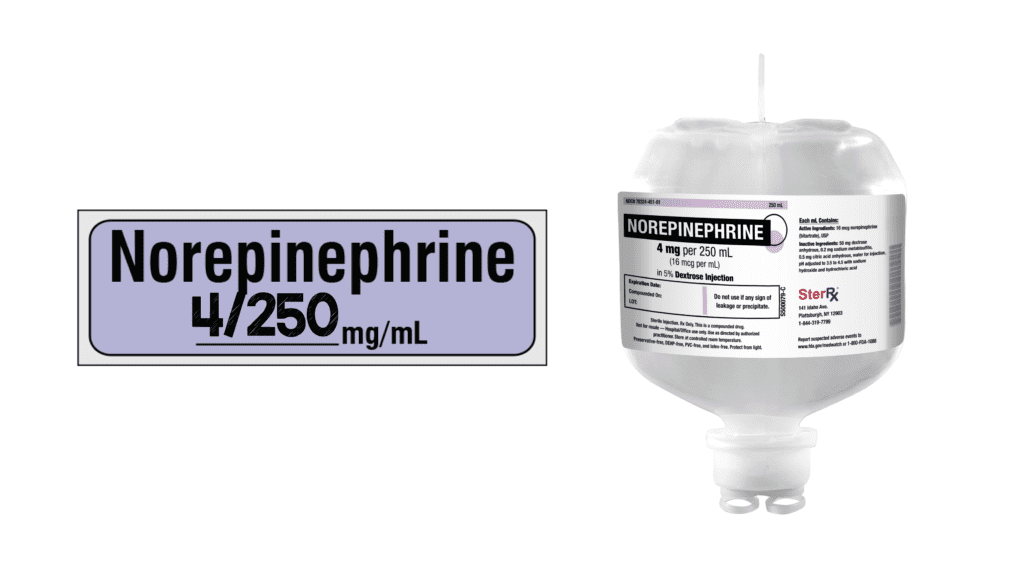
Pearl #4: Use a Dilute Concentration + Small Volume
- Norepinephrine comes in 4mg, 8mg, and 16mg doses. Use the smallest dose which is 4mg
- You can mix the norepinephrine in a variety of fluids. This does not matter as much as the volume you mix it in (This should be 250mL)
Pearl #5: Have an Observation Protocol
- Once you have started an infusion through a peripheral IV, someone should be physically visualizing the site q15 to q30min. This ensures that if extravasation occurs it is as small a volume as possible to avoid ischemia and necrosis of the extremity
Pearl #6: Have an Extravasation Protocol [3]
- If extravasation occurs, stop the infusion and switch it to a different line
- Leave the catheter in place
- Suck out as much as you can from the catheter
- Use Phentolamine or Terbutaline (Whichever you have available):
- Phentolamine
- 5mg/mL x2 in 8mL of NS (Max 10mg)
- Inject 5mL through catheter
- Inject remaining 5mL in the subq tissue (Around area of blanching)
- Unclear what time frame is optimal for re-dosing (Typically wait 1hr)
- Terbutaline
- 1mg/mL in 9mL of NS
- Inject 5mal through catheter
- Inject remaining 5mL in the subq tissue (Around area of blanching)
- Can repeat every 15min as needed
- Nitroglycerin
- Apply 1inch of topical paste to the affected area
- Can repeat every 8 hours
- Elevate the extremity
- Use warm compress (Be careful to not burn the skin)
- Phentolamine
Clinical Bottom Line:
- Use an antecubital fossa or more proximal vein (Larger diameter)
- Use an ultralong catheter (6.35cm or 2.5in — >2.5cm in the vein)
- Do not run infusions for >2 – 4hrs
- Use as dilute a concentration in as small a volume as possible (4mg/250mL)
- Have an IV observation protocol (q15 – q30min)
- Have an extravasation protocol (Phentolamine or Terbutaline + Topical NTG + Elevation + Warm Compress)
References:
- Tian DH et al. Safety of Peripheral Administration of Vasopressor Medications: A Systematic Review. EMA 2019. PMID: 31698544
- Pancaro C et al. Risk of Major Complications After Perioperative Norepinephrine Infusion Through Peripheral Intravenous Lines in a Multicenter Study. Anesth Analg 2019. PMID: 31569163
- Lewis T et al. Safety of the Peripheral Administration of Vasopressor Agents. J Intensive Care Med 2019. PMID: 28073314
- Loubani OM et al. A systematic review of extravasation and local tissue injury from administration of vasopressors through peripheral intravenous catheters and central venous catheters. J Crit Care 2015.PMID: 25669592
- Medlej K et al. Complications from Administration of Vasopressors Through Peripheral Venous Catheters: An Observational Study. JEM 2018. PMID: 29110979
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami) and Mizuho Morrison, DO (Twitter: @mizuhomorrison)
The post Peripheral Pressors: 6 Pearls to Not F*#k Up the Arm appeared first on REBEL EM - Emergency Medicine Blog.