
Background Information: The successful placement of an endotracheal tube (ETT) is a necessary skill all emergency physicians must possess. Performing life-saving interventions are understandably stressful as their failure can lead to morbid consequences and expedited patient death.1,2 The intensive training of emergency physicians, the availability of multiple alternative airway adjuncts and the use of rapid-sequence intubation has helped reduce the intubation complication rate among trauma and medical patients.3-5 Confirmatory methods to ensure the placement of the endotracheal tube are ever changing with no single method being infallible.6. Physical exam findings such as auscultation of the chest and epigastrium, visualization of thoracic movement and fogging of the ETT are not sufficiently reliable to confirm placement.7,8 The use of end-tidal CO2 detection has been shown to have a cumulative false-positive and false-negative failure rate of 10% in accurately confirming the ETT’s location according to the authors of this paper (The paper referenced is a bit dated).6 Furthermore, the usage of these devices may contribute to the complications as they frequently require up to 5 ventilations to obtain an accurate reading.9-11 This puts the patient at risk for aspiration especially if the tube is in the esophagus. No.12 Despite a post-intubation CXR taking time, exposing the patient to more radiation and adding to the cost of treatment, it still continues to remain the standard of care.12-14 The authors of this study wished to better understand the test characteristics of utilizing ultrasound to confirm ETT placement. They conducted a systematic review and meta-analysis to quantify the accuracy of this ETT confirmatory method.
Clinical Question:
- Using a systematic review and meta-analysis of the current literature, what is the diagnostic accuracy of using ultrasonography to confirm endotracheal tube placement?
What They Did:
- This was a systematic review and meta-analysis of prospective and randomized control trials between 2007 and 2017 related to the use of ultrasonography to confirm ETT tube placement using PubMed, Scopus, CINAHL, LILACS, Cochrane Database of Systematic Reviews and the Cochrane Central Register of Controlled Trials. Two investigators independently assessed the studies for eligibility based on the criteria below and the duplicates were removed.
Inclusion Criteria:
- All prospective or randomized control trials assessing transtracheal ultrasonography for endotracheal tube placement confirmation in adult patients older than 18 years old without language or date restrictions
- All studies must have had a confirmatory test such as
- End-tidal capnography
- Colorimetric capnography
- Direct visualization
Exclusion Criteria:
- The following were excluded from review:
- Case reports
- Case series
- Retrospective studies
- Cadaver studies
- Pediatric studies
- Conference abstracts
Outcomes:
Primary:
- Diagnostic accuracy of transtracheal ultrasonography
Subgroup Analysis:
- Location (ED vs Non-ED)
- Provider Specialty (Emergency vs non-emergency)
- Provider experience (Attending vs non-attending physician)
- Transducer type (Linear vs curvilinear)
- Technique (Static vs dynamic)
- Static: Evaluating the ETT location after the intubation attempt
- Dynamic: Evaluating the ETT location in real-time during the intubation attempt
Secondary:
- Time to confirmation of endotracheal tube using ultrasonography.
-
- This was calculated from the when the laryngoscope entered the mouth (signaling the start of the intubation attempt) to the moment the endotracheal tube was visualized on ultrasound.
Results:
- A total of 6220 records screened and 6123 were excluded.
- Of those 97 full text articles, 80 were excluded and the remaining 17 were included the qualitative and quantitative synthesis
- The 17 studies were performed across 8 countries between 2007 and 2017.
- 1595 total patients with a mean age of 55
- Population sizes ranging from 30 to 150 patients
- 15 studies were prospective observation trials
- 2 studies were randomized control trials
- 12 studies were conducted in the ED and the other 5 in the operating room
- 8 studies used the dynamic technique while 9 used the static technique
- The sonographers were emergency physicians in 13 of the studies, anesthesiologists in 3 studies and in one study the specialty was not described
Critical Results:
Table 1: Results for confirmation of the ETT using transtracheal ultrasonography
- The area under the receiving operating characteristic (AUROC) curve indicated high accuracy (0.994; CI 0.982 to 0.998)
- Overall esophageal intubation rate was 15.3%
- There was no significant difference in accuracy between the studies with respect to training protocol used, ultrasound technique (static vs dynamic), or sonographer experience (medical student vs ultrasound fellowship trained attending physicians)
- Overall mean time to confirmation was 13.0 seconds
Strengths:
- Utilized several different medical databases to identify as many studies as possible
- The exclusion of case reports and case series helped make the review less anecdotal and more evidence based. Furthermore, the exclusion of cadaver studies made the review more clinically relevant
- The authors made sure to include a wide variety of factors in the subgroup analysis
- Had a large and internationally diverse total patient population across the 17 studies
- Used several statistical tests to analyze the data and confirm their findings
- The authors recognized factors that would contribute to bias and therefore created a funnel plot and a linear regression test to further evaluate its asymmetry
- Looked at the pros and cons of two previous systematic reviews and meta-analyses performed on this topic. When compared to those studies this review used a broader and more updated search strategy. They also made sure to exclude cadaver and non-transtracheal ultrasonographic techniques. As a result, they identified 9 additional studies with less heterogeneity in the findings and nearly twice as many patients than the previous review.
Limitations:
- Disproportionate inclusion of true negative results across studies suggests a possible publication bias
- On the topic of bias, 13 of the 17 studies used convenience sampling which creates a bias for patient selection.
- Most of the studies had small sample sizes which resulted in wide confidence intervals
- There were significant variations in the sonographer training protocols across the different studies making it difficult isolate one or two that were particularly useful and effective for confirming ETT.
- The authors do not identify any information within the studies regarding intubation attempts or difficult airways which may serve to be confounding variables.
- In addition to the above, the studies do not further elaborate on the exact position of the ETT (ie. Right-sided bronchus, main-stem bronchus, etc) or utilize any other ultrasound driven confirmatory techniques such as lung-sliding.
- Furthermore, the authors do not investigate within the studies which intubation attempt ultrasound was used. This may introduce a reporting bias as studies are less likely to report the use of ultrasound if it was the third-plus attempt at intubation.
- The authors focus on immediate ETT confirmatory methods and do not mention more common modalities such as chest x-ray or clinical response
- 13 of the 17 studies had an “unclear risk of bias” which was not further elaborated on
- 15 of the 17 studies were observational and the remaining two were RCTs
- Roughly half of the studies were performed over 5 years ago when ultrasonography was not as popular and less utilized. A review of more recent studies may lead to different results
Discussion:
- When compared to a previous meta-analysis of capnography, the results of this study suggest that ultrasonography is more sensitive and with similar specificity.6
- A previous study found the confirmation of ETT placement using auscultation combined with capnography to take 48 seconds.17 The secondary findings of this study suggests that isolated transtracheal ultrasonography may be nearly 4 times faster.
- The authors advocate for the use of ultrasound over other confirmatory methods since it is faster, more readily available, non-invasive and does not require multiple ventilations to confirm its placement.
- Training and sonographer experience is an important factor that is not emphasized enough in this study. While the authors state there was no significant difference in the accuracy between studies with respect to the training protocol used, the clinical significance of sonographer experience is worth highlighting. In the time-sensitive setting immediately following intubation, the most experienced sonographer should be the one to confirm the ETT. We agree with the authors that the providers should obtain sufficient training and receive targeted feedback before utilizing ultrasound to guide clinical decisions.
- While we agree with the authors that ultrasound should not be used for every intubation confirmation, we do recommend having the ultrasound at bedside whenever an intubation is about to be performed. It serves as a time-saving step should there be any complications such as a peri-intubation arrest.
- Often space is limited for hospital personnel during critical airway management and this may be the cause of some hesitation to wheeling in another piece of equipment into a tight space. The use of ultrasound for ETT confirmations serves to be useful when another team member is intubating (ie. Resident, CRNA, etc) and is particularly helpful during a cardiac arrest when it is not possibly to obtain a CXR.
- The authors emphasize caution when placing the transducer on the trachea during intubation as this can make an intubation attempt more difficult. Factors that may preclude sonographic use include: large neck masses, abnormal upper airway anatomy, soft tissue air, cervical collars, or significant neck edema.
- A future study, that may serve to be more clinically relevant, would be to identify which of the three signs is the most accurate when using ultrasound to confirm the ETT.
Author’s Conclusions:
- Transtracheal sonography is a valuable adjunct with an acceptable degree of sensitivity and specificity for ETT confirmation. It should be considered when quantitative capnography is unavailable or unreliable.
Our Conclusion:
- Confirmation of the ETT should be done using multiple techniques as no one singular method is perfect. With that said, Ultrasonography is another useful tool for confirming ETT placement when used in the hands of an experienced and well-trained sonographer. Judicious use is required as it may not be appropriate for all intubations and more importantly should not add to the difficulty of placing an ETT. The use of ultrasound should be considered in conjunction with other confirmatory methods such as but not limited to the following: chest and epigastric auscultation, end-tidal capnography, ETT condensation, visualization of chest expansion, clinical improvement, and chest x-ray.
Expert Peer Review By:
IMAGES:
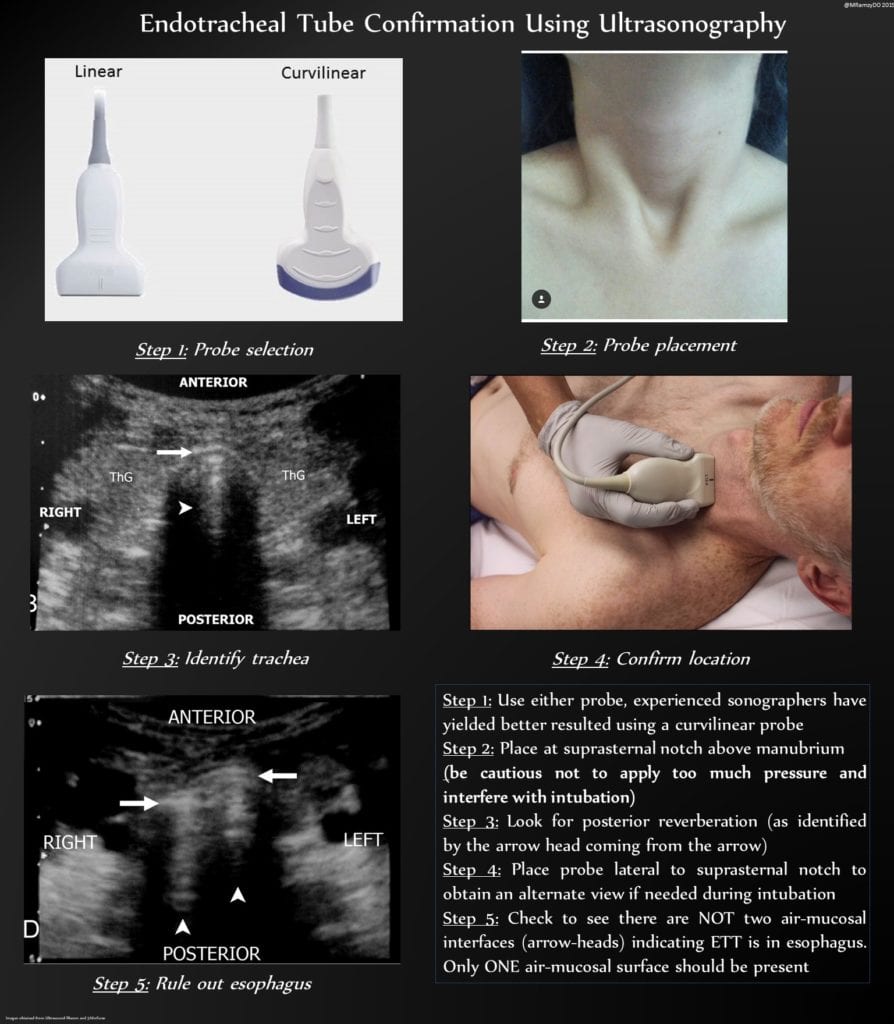
Image 1: Step by Step guide on using ultrasound for ETT confirmation

Image 2: Double Tract Sign. Image from Favot M, ALiEM 2015: Ultrasound for Verification of ETT

Image 3: Triangle Sign. Image from Abbasi et al. EJEM 2015 PMID: 24441884
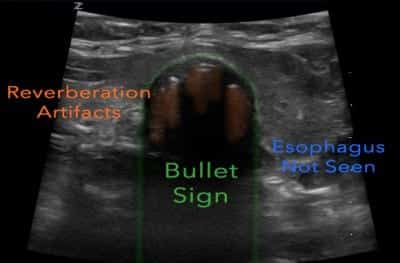
Image 4: Bullet Sign. Image from Favot M, ALiEM 2015: Ultrasound for Verification of ETT
REFERENCES:
- Gottlieb M,et al. Ultrasonography for the Confirmation of Endotracheal Tube Intubation: A Systematic Review and Meta-Analysis. Ann Emerg Med. 2018. PMID: 30119943
- Clyburn P et al. Accidental oesophageal intubation. Br J Anaesth. 1994. PMID: 8038057
- American College of Emergency Physicians. Rapid-sequence intubation [position statement 400177], 1996. Link here
- American College of Surgeons, Advanced trauma life support for doctors, 6th edn, ACS, Chicago. 1997. Link here
- Li J, et al. Complications of emergency intubation with and without paralysis. Am J Emerg Med, 1999. PMID: 10102312
- Li J, Capnography alone is imperfect for endotracheal tube placement confirmation during emergency intubation. J Emerg Med. 2001. PMID: 11267809
- Kelly JJ et al.Use of tube condensation as an indicator of endotracheal tube placement. Ann Emerg Med. 1998. PMID: 9581141
- American College of Emergency Physicians Board of Directors. Verification of Endotracheal Tube Placement. policy statement. Revised April 2009.
- MacLeod BA, et al. Verification of endotracheal tube placement with colorimetric end-tidal CO2 detection. Ann Emerg Med. 1991. PMID: 1899985
- Takeda T, et al. The assessment of three methods to verify tracheal tube placement in the emergency setting. Resuscitation. 2003. PMID: 12589988
- Milling TJ, et al. Transtracheal 2-d ultrasound for identification of esophageal intubation. J Emerg Med. 2007. PMID: 17499696
- McGillicuddy D et al. Is a postintubation chest radiograph necessary in the emergency department?. Int J Emerg Med. 2009. PMID: 20436895
- W. Brunel, et al. Assessment of routine chest roentgenograms and the physical examination to confirm endotracheal tube position Chest. 1989. PMID: 2509149
- Hossein-Nejad H, et al. Chest radiography after endotracheal tube placement: is it necessary or not?. Am J Emerg Med. 2013. PMID: 23810228
- Favot M, Ultrasound for Verification of Endotracheal Tube Location. ALiEM. Link Here
- Abbasi S, et al. Direct ultrasound methods. European Journal of Emergency Medicine. 2015. PMID: 24441884
- Pfeiffer P, et al. Temporal comparison of ultrasound vs auscultation and capnography in verification of endotracheal tube placement. Acta Anaesthesiol Scand. 2011. PMID: 22260400
For More on this Topic Checkout:
- Ultrasound G.E.L. Podcast: Tracheal Ultrasound for Intubation
- Academic Life in Emergency Medicine: Ultrasound for Verification of Endotracheal Tube Location
- The SGEM: SGEM #249 – Ace in the Hole – Confirming Endotracheal Tube Placement with POCUS
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post POCUS for Endotracheal Tube Confirmation appeared first on REBEL EM - Emergency Medicine Blog.