
 Background: The clinical diagnosis of pulmonary embolism (PE) can be challenging given its variable presentation, thus requiring dependence on objective testing. Decision instruments such as PERC and the Wells’ score help stratify patients to low or high probability, enabling focused use of CT pulmonary angiography (CTPA) for diagnosis. However, despite these algorithms, there is evidence of increasing use of CTPA along with diminishing diagnostic rate (less than 10%). This combination results in the overdiagnosis of subsegmental PEs, unnecessary exposure to radiation and false positive results. These issues are compounded in patients with pregnancy. While we know that pregnancy increases risk of venous thromboembolism (VTE) our testing rates far exceed the added risk exposing thousands of women to the afore mentioned potential harms.
Background: The clinical diagnosis of pulmonary embolism (PE) can be challenging given its variable presentation, thus requiring dependence on objective testing. Decision instruments such as PERC and the Wells’ score help stratify patients to low or high probability, enabling focused use of CT pulmonary angiography (CTPA) for diagnosis. However, despite these algorithms, there is evidence of increasing use of CTPA along with diminishing diagnostic rate (less than 10%). This combination results in the overdiagnosis of subsegmental PEs, unnecessary exposure to radiation and false positive results. These issues are compounded in patients with pregnancy. While we know that pregnancy increases risk of venous thromboembolism (VTE) our testing rates far exceed the added risk exposing thousands of women to the afore mentioned potential harms.
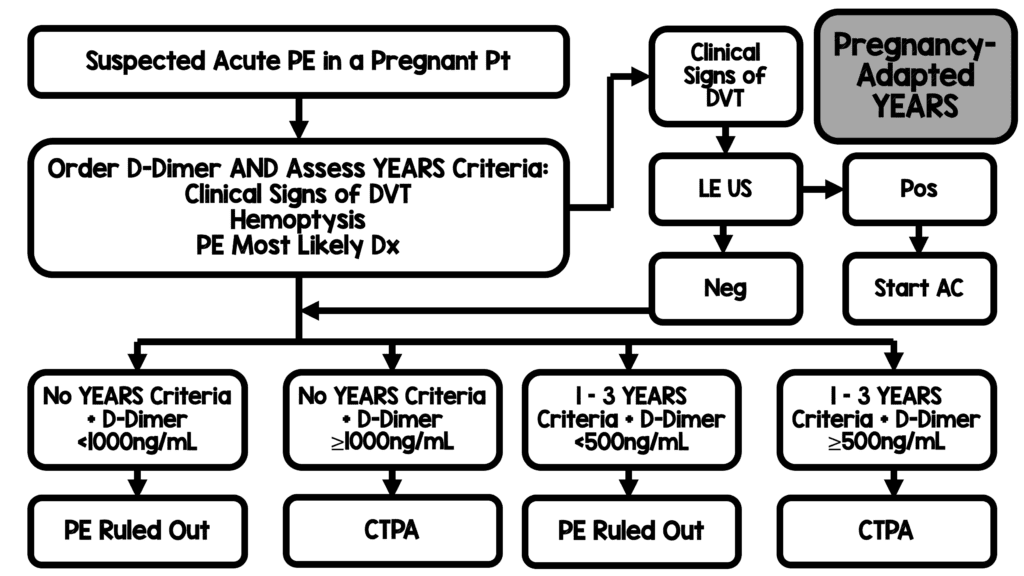
In 2017, the YEARS algorithm established a simplified algorithm for evaluation with a two-tiered D-dimer threshold in an effort to reduce the number of patients getting CTPA (van der Hulle 2017). The YEARS algorithm asks three questions: 1) Are there clinical signs of DVT? 2) Does the patient have hemoptysis? and 3) is PE the most likely diagnosis. If the answer to all 3 questions is no, the D-dimer threshold is set at 1000 ng/mL FEU (500 ng/mL DDU) and if the answer is “yes” to any of the 3 questions, the D-dimer threshold is set at 500 ng/mL (250 ng/mL DDU). However, this study had very few pregnant women enrolled.
Clinical Question: Can a pregnancy-adapted YEARS algorithm safely avoid diagnostic imaging in pregnant women with suspected pulmonary embolism?
Article: van der Pol LM et al. Pregnancy-Adapted YEARS Algorithm for diagnosis of Suspected Pulmonary Embolism. NEJM 2019; 380(12): 1139-49. PMID: 30893534
Population: Pregnant women > 18 years of age who had been referred to the ED or obstetrical ward for suspected PE defined as new or worsening chest pain or dyspnea with or without hemoptysis or tachycardia
Primary Outcome: Cumulative incidence of symptomatic VTE during a 3-month follow-up period in subgroup of patients in whom anticoagulation treatment was withheld on the basis of a negative YEARS algorithm
Secondary Outcome: Proportion of patients being evaluated for PE who did not require a CTPA based on the algorithm
Design: Prospective, multicenter, observational study conducted at 11 academic and 7 nonacademic hospitals.
Excluded: Treatment with a full therapeutic dose of anticoagulant initiated > 24 hours before enrollment, unavailability of patient for follow-up, allergy to iodinated contrast enhancement, life expectancy of 3 months or less
Note: The adaptation of the YEARS algorithm in pregnant women was simply that Compression US was performed in all women with symptoms of DVT and if positive, CTPA was not performed.
Pregnancy-Adapted YEARS Algorithm
Primary Results:
- 510 women were screened
- 12 (2.4%) of women screened were excluded
-
498 patients ultimately evaluated in this study
- 46% of patients in 3rd trimester of pregnancy
Critical Findings:
-
- Total number of VTE: n = 20 (4.0% 95% CI 2.6 – 6.1)
- YEARS criteria negative 51% (n = 252)
-
YEARS criteria positive 49% (n = 246)
-
YEARS Features
- Hemoptysis: 7.7% (n = 19)
-
Signs of DVT: 19% (n = 47)
- 7% (n = 3) + DVT study
- PE considered most likely diagnosis 89% (n = 218)
-
YEARS Features
-
D-Dimer Testing
- 39% (n = 195) below threshold for further testing
-
61% (n = 299) above threshold (required further testing)
- CTPA (n = 273) positive in 15 patients
- V/Q Scan (n = 2) positive in 1 patient
- Protocol violation: 24 patients had no imaging
- 1 patient was YEARS criteria negative but D-Dimer +
-
Primary Outcome (VTE at 3 months)
-
n = 477 (96%) PE ruled out at baseline
- n = 476 with no symptomatic VTE at 3 months
-
n = 1 VTE during follow up 0.21% (95% CI -.04 – 1.2)
- Patient had symptomatic popliteal DVT diagnosed on day 90
-
n = 477 (96%) PE ruled out at baseline
-
Secondary Outcome
- n = 195 patients who were ruled out based on adapted YEARS
-
n = 12 (6.2%) underwent CTPA (protocol violation)
- All 12 negative for PE
- CTPA could safely be avoided in 39% of patients (95% CI 35-44)
Strengths:
- Study asks a clinically important question addressing a shortcoming of the parent study (i.e. original YEARS study had very few pregnant women enrolled)
- Multicenter study increasing external validity
- Screened patients consecutively for enrollment
- Follow up was excellent with only 1 patient temporarily lost to follow up (ultimately, was found)
- Enrolled women in 1st, 2nd, and 3rd trimester of pregnancy
- An independent committee assessed and adjudicated all suspected cases of VTE and deaths that occurred during follow up
Limitations:
- Only enrolled patients in Netherlands and France decreasing external validity
- All patients were not tested for VTE and, thus, some VTE may have been missed
- All hospitals used D-dimer assays using FEU (no mention of assays using DDU)
- Protocol violations were present and in greater numbers in group in which algorithm directed clinicians towards CTPA
- Due to the parallel timing of the assessment of YEARS criteria and the measurement of the D-Dimer level, physicians may have occasionally been aware of the D-Dimer result when they were assessing the YEARS criteria which may have biased the evaluation of patients
- Patients underwent 2-point compression ultrasonography of the deep veins of the symptomatic leg (at the popliteal and inguinal levels) to confirm or rule out proximal DVT. Using this strategy may have missed some DVTs between these two areas.
Discussion:
- Study adaptation was pragmatic – pregnant women with confirmed DVT do not require CTPA since it would not change management but would expose the patient and fetus to radiation
- YEARS criteria are simple to remember as there are only 3 of them and the D-Dimer cutoffs are simple as well
- Not all patients had a CTPA performed and, thus, some PEs may have been missed. However, the lack of symptoms prompting further assessment and diagnosis of VTE at 3 months in almost all patients means that PEs missed were very likely to be clinically irrelevant
- The overall prevalence of VTE was low in this cohort (~ 4%) but, the rate is consistent with prior published reports that have shown a prevalence of PE of <5% among pregnant patients in whom PE is suspected, as compared to 15 – 20% in non-pregnant patients
- It would be interesting to add a trimester-adjusted d-dimer threshold to this algorithm (UMEM Pearls) which could further reduce the need for CTPA
- The efficiency of the algorithm was highest during the first trimester of pregnancy and the lowest during the third trimester of pregnancy; CTPA was avoided in 65% who began the study in the first trimester of pregnancy and in 32% who began the study in the third trimester of pregnancy
- The definition of PE was a new filling defect in a subsegmental or more proximal pulmonary artery, however, sub segmental PEs may be clinically insignificant
-
One of the three YEARS criteria is subjective in nature – “PE as the most likely diagnosis”
- This subjective criterion makes application more challenging
- Most common feature of those who had > 1 YEARS criteria (89%)
- Difficult to know if gestalt of this group of clinicians is similar to overall gestalt
- In countries were testing is more conservative (i.e. US) the reduction in testing may be less dramatic because of this
Authors Conclusions: “Pulmonary embolism was safely ruled out by the pregnancy-adapted YEARS diagnostic algorithm across all trimesters of pregnancy. CT pulmonary angiography was avoided in 32 to 65% of patients.”
Our Conclusions: Overall, we agree with the authors conclusions. The pregnancy-adapted YEARS algorithm safely ruled out PE in this cohort of patients with a small risk of VTE at 3 months if the patient was negative on initial visit.
Potential to Impact Current Practice: External validation of this approach is needed but, application of the pregnancy-adapted YEARS algorithm has the potential to safely decrease CTPA use in pregnant women in whom the clinician has a concern for PE.
Bottom Line: The Pregnancy-Adapted YEARS algorithm has both face validity and is pragmatic for clinical practice. However, before implementation of this algorithm into everyday practice, an external validation study would be warranted.
For More on this Topic Checkout:
- REBEL EM: The YEARS Study – Simplified Diagnostic Approach to PE
- REBEL EM: D-dimer and Pregnancy: The DiPEP Study
- UMEM Educational Pearls: Ruling Out Pulmonary Embolism During Pregnancy
- The SGEM: In the Pregnant YEARS – To Rule Out VTE
- The Breach: YEARS for Suspected PE in Pregnancy
References:
- van der Hulle T et al. Simplified diagnostic management of suspected pulmonary embolism (the YEARS study): a prospective multicentre, cohort study. Lancet 2017; 390: 289-97. PMID: 28549662
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post Pregnancy-Adapted YEARS Algorithm for PE – Ready for Prime Time? appeared first on REBEL EM - Emergency Medicine Blog.