 A 55 year old male was brought to the Emergency Department (ED) by paramedics complaining of weakness and chest discomfort. His past medical history was notable for coronary artery disease with bypass grafting, diabetes mellitus, and end stage renal disease. He reported being non-compliant with his last 2 scheduled hemodialysis sessions. Paramedics noted pallor and recorded a blood pressure of 80/palpated and a heart rate of 44. Upon arrival to the ED, a 12 lead ECG was obtained.
A 55 year old male was brought to the Emergency Department (ED) by paramedics complaining of weakness and chest discomfort. His past medical history was notable for coronary artery disease with bypass grafting, diabetes mellitus, and end stage renal disease. He reported being non-compliant with his last 2 scheduled hemodialysis sessions. Paramedics noted pallor and recorded a blood pressure of 80/palpated and a heart rate of 44. Upon arrival to the ED, a 12 lead ECG was obtained.

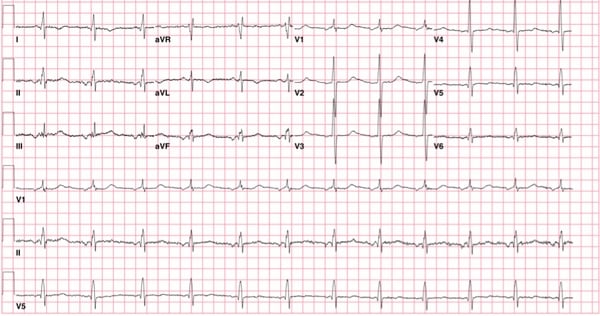
ECG Interpretation: Ectopic atrial rhythm, ventricular rate of 40, with AV delay and a widened QRS complex in a RBBB pattern. Right axis deviation and an irregular ventricular rate.
Given the weakness, chest pain, and hypotension, a broad differential diagnosis was considered including ACS, cardiac tamponade, primary arrhythmia, pulmonary embolus, electrolyte disturbance, or central nervous system catastrophe.
Cardiac monitoring was initiated and preparation for transcutaneous pacing was made due to symptomatic bradycardia. Due to the history of missing dialysis, hyperkalemia was suspected and stat laboratory testing confirmed a K+ of 8.8 mmol/L. Intravenous calcium gluconate was given and a renal consultation was requested for hemodialysis.
Clinical Questions
- What are the classic ECG manifestations of hyperkalemia?
- What ECG findings of hyperkalemia are not commonly recognized?
Evolution of ECG findings with hyperkalemia
The earliest, classic electrocardiographic sign of hyperkalemia is reported to be tall, narrow based, symmetric T wave, bearing a sharp point. This is the so-called “peaked” T wave.

For reference, T wave amplitude is normally less than 0.5 mV (5 mm) in the limb leads and 1.5 mV (15 mm) in the precordial leads.[1]
As the serum potassium rises, the following ECG findings are classically found in sequential order with rising levels:[2-4]
- Lengthening of the P-R interval and a reduction of P wave amplitude
- Widening of the QRS complex
- Various intraventricular conduction abnormalities including atypical bundle branch blocks
- “M” shaped QRS-ST-T complex
- Without intervention, a sine-wave pattern, ventricular fibrillation (VF) or asystole develops.
Sensitivity and specificity of ECG findings
Unfortunately, the ECG is neither sensitive nor specific as a tool for determining the serum potassium concentration.[5,6] In a study of experienced acute care physicians, the sensitivity of the ECG for hyperkalemia was at best 0.43 and specificity was 0.86.[5] In the same study, the sensitivity of the ECG was still low at 0.62 when limited to those patients with a K+ greater than 6.5 mmol/L.
Furthermore, it has been demonstrated that the ECG is particularly insensitive to elevations in potassium concentration in patients with end stage renal disease.[7,8] This places such patients at risk as practitioners may depend on the classic findings of hyperkalemia and may be reassured in the absence of these findings even in the presence of marked elevations of potassium concentration.

In this case, marked bradycardia with a ventricular rate of 40, AV delay, and a prolonged QRS complex of 126 msec was present. Interestingly, the T waves were broad based and not tall (above image), which may have falsely reassured the clinician as not being “peaked”. Don’t fall into that trap!
Continuation of the Case
Before hemodialysis could be initiated, the patient had a VF arrest. He was resuscitated with countershock followed by multiple rounds of intravenous calcium gluconate, insulin, and dextrose. In the intensive care unit, the patient stabilized with dialysis. The repeat K+ was 4.2 mmol/L, and an ECG was recorded the next day:
As demonstrated in this case, bradycardia is a common presentation in the acute care setting. It is critical that practitioners treat bradycardia with or without the other classic ECG findings of hyperkalemia aggressively with close cardiac monitoring to prevent ventricular fibrillation and cardiac standstill. This fact is incompletely emphasized in textbooks and papers describing the treatment of hyperkalemia.
Teaching Points
- The ECG is neither sensitive nor specific as a tool for determining the serum potassium concentration, especially in patients with end stage renal failure.
- Peaked T waves are not reliably seen in severe hyperkalemia.
- Bradycardia in the setting of hyperkalemia is ominous and should be treated aggressively.
[bg_faq_start]
References
- Wagner, GS. Marriott’s practical electrocardiography-11th ed. 2008. Lippincott Williams and Wilkins. Philadelphia, PA.
- Ahmed J, Weisberg L: Hyperkalemia in dialysis patients. Semin Dial 2001. 14: 348–356.
- Surawicz B. Relationship between electrocardiogram and electrolytes. Am Heart J. 1967. Jun;73(6):814-34.
- Fisch C. Relation of electrolyte disturbances to cardiac arrhythmias. Circulation 1973;47: 408-419.
- Wrenn KD, Slovis CM, Slovis BS: The ability of physicians to predict hyperkalemia from the ECG. Ann Emerg Med.1991;20: 1229-1232.
- Montague BT, Ouellett JR, Buller GK. Retrospective review of the frequency of ECG changes in hyperkalemia. Clin J Am Soc Nephrol 2008; 3: 324-330.
- Aslam S, Friedman EA, Ifudu O. Electrocardiography is unreliable in detecting potentially lethal hyperkalaemia in haemodialysis patients. Nephrol Dial Transplant 2002 17: 1639–1642.
- Martinez-Vea A, Bardaji A, Garcia C, Oliver JA. Severe hyperkalemia with minimal electrocardiographic manifestations: a report of seven cases. J. Electrocardiol. 1999 Jan; 32(1): 45-9.
[bg_faq_end]
Disclaimer: The cases in this series are very loosely based on an aggregate pool of known patient cases from around the country over the past decade, although the lessons are timeless.
Author information

The post QI Series: Pitfalls in Diagnosing Hyperkalemia appeared first on ALiEM.