
 Background: Acute atrial fibrillation (AF) is one of the most common dysrhythmias seen in the emergency department (ED). There has been extensive discussion and debate about the best way to manage acute AF centered around rate and rhythm control. However, there is little data to guide the optimal approach to rhythm control once this option is selected. As a result of the absence of good evidence, there is significant variation in management. Better data is integral to establishing best practices. The RAFF2 randomized trial attempted to provide more data on this debate of electrical vs pharmacological cardioversion in patients with acute atrial fibrillation/flutter.
Background: Acute atrial fibrillation (AF) is one of the most common dysrhythmias seen in the emergency department (ED). There has been extensive discussion and debate about the best way to manage acute AF centered around rate and rhythm control. However, there is little data to guide the optimal approach to rhythm control once this option is selected. As a result of the absence of good evidence, there is significant variation in management. Better data is integral to establishing best practices. The RAFF2 randomized trial attempted to provide more data on this debate of electrical vs pharmacological cardioversion in patients with acute atrial fibrillation/flutter.
Paper: Stiell IG et al. Electrical Versus Pharmacological Cardioversion for Emergency Department Patients with Acute Atrial Fibrillation (RAFF2): A Partial Factorial Randomised Trial. Lancet 2020. PMID: 32007169
Clinical Question: Is a pharmacological cardioversion first approach more successful than an electrical cardioversion first approach in acute atrial fibrillation?
What They Did:
- Recent-onset Atrial Fibrillation/Atrial Flutter (RAFF2)
- Partial factorial trial of two protocols for patients with acute atrial fibrillation at 11 academic hospital EDs in Canada
-
Protocol 1:
- Randomized, blinded, placebo-controlled comparison of attempted pharmacological cardioversion with IV procainamide (15mg/kg in 500mL of 0.9% saline over 30min with max dose of 1500mg) followed by electrical cardioversion if necessary (up to 3 shocks, each at ≥200J) vs placebo infusion followed by electrical cardioversion
-
Protocol 2 (Patients getting electrical cardioversion):
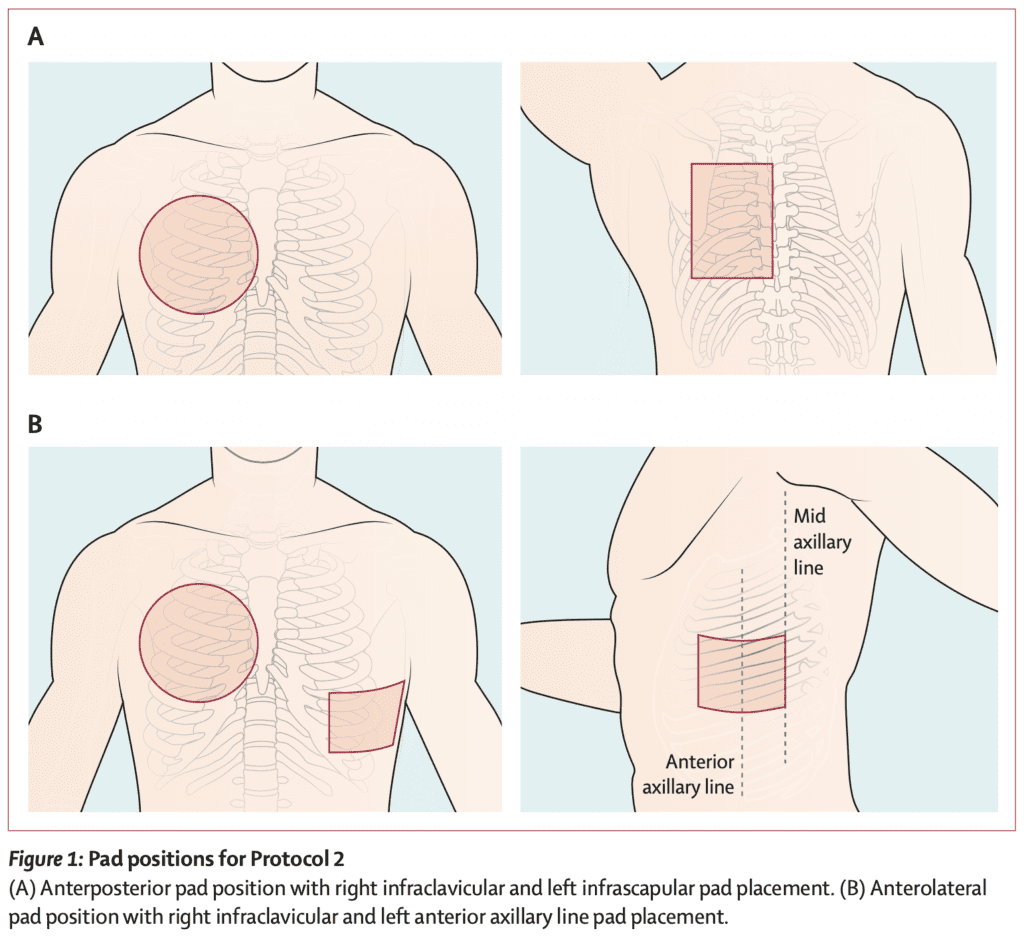
- Randomized, open-label, nested comparison of anteroposterior vs anterolateral pad positions

Outcomes:
- Primary: Conversion to normal sinus rhythm for at least 30 min at any time
-
Secondary:
- Cardiac rhythm at disposition
- Length of stay in the ED
- Adverse events
Inclusion:
- Hemodynamically stable patients with a primary diagnosis of acute atrial fibrillation of at least 3h duration
- Acute atrial fibrillation = Clear history of onset within 48h of arrival to the ED, onset within 7d of arrival and adequately anticoagulated for at least 4 weeks, or onset within 7d of arrival and no left atrial thrombus on transesophageal echocardiography
- Symptoms necessitated early management
- Pharmacological or electrical cardioversion appropriate option
Exclusion:
- Unable to give consent
- Permanent atrial fibrillation
- Hemodynamical unstable requiring immediate cardioversion
- Hemodynamically unstable = SBP <100mmHg, rapid ventricular pre-excitation, acute coronary syndrome, or pulmonary edema
- Primary presentation for another condition: (i.e. pneumonia, pulmonary embolism, sepsis)
- Converted spontaneously before randomization
- Previously enrolled in the study
- Known heart failure (LVEF <30% or clinical or radiological evidence of acute heart failure
- Heart rate <55BPM
- 3rd degree AV block or complete LBBB
- Brugada syndrome
- Currently taking class I or III antiarrhythmic drugs other than amiodarone
- Hypersensitivity to procainamide
- Recent MI (<3 months)
- End stage liver disease
- Breast feeding or pregnant
Results:
- 396 patients enrolled
- Drug-shock group: 204 patients
- Shock only group: 192 patients
-
Conversion to NSR (Primary Outcome):
- Drug-Shock: 96%
- Shock Only: 92%
- Absolute Difference 4.0%; 95% CI 0 to 9; p = 0.07
- 52% of patients in the drug-shock group converted after drug infusion only vs 9% in the shock only group
- No difference in mean total ED LOS: 7.1hr vs 7.6hr
- No serious adverse events in either group
- At 14d follow up 95% of patients were in NSR on ECG
- Discharged Home:
- Drug-Shock: 97%
- Shock Only: 95%
- P = 0.60
- Conversion to NSR based on Pad Position:
- Anteroposterior: 92%
- Anterolateral: 94%
- RR 1.01; 95% CI 0.95 to 1.09; P = 0.68
- Most patients converted after one shock (88% vs 81%)
Strengths:
- Asked an important clinical question with minimal prior research
- No loss to follow up (all patients enrolled were accounted for)
- Electrophysiologist, blinded to group assignment adjudicated initial ECG to verify that rhythm was atrial fibrillation
- Patients, research staff, and ED staff were masked to group assignment
- Discussions with hospital staff confirmed that staff were unable to identify the fluid in each bag
- Patients re-assessed in person by research personnel at 14d to determine cardiac rhythm, return visits to the ED, stroke, and survival
- Primary analytical approach for Protocol 1 included the intention-to-treat principle and a secondary modified intention-to-treat analysis that excluded patients who converted to sinus rhythm before the study infusion was started
- Performed multiple logistic regression analysis to account for potential confounders which were chosen a priori to verify the precision of the results
- Groups were fairly balanced at baseline for demographics and clinical characteristics
Limitations:
- Study was 90% powered to detect a 10% difference. This may have been overly ambitious
- This appears to be a convenience sample, as opposed to a consecutive sample which could bias results. Of 11,096 patients screened 210 were not approached for inclusion in the trial, which could change the results of the study
- Many patients (582 in fact) refused participation most often because they had a strong preference for pharmacological or electrical cardioversion
- Other pharmaceutical options such as flecainide or propafenone were not studied
- Thromboembolic events after cardioversion are rare. It would require a much larger study to show more clearly who can safely be cardioverted without need for anticoagulation
Discussion:
- Knowing inclusion/exclusion criteria is critical in evaluating literature. A key exclusion in this study is a primary presentation for another condition: (i.e. pneumonia, pulmonary embolism, sepsis, etc…). This paper is essentially about lone atrial fibrillation/flutter and we have to be careful extrapolating to groups not included in the trial
- In patients receiving infusion the medication was stopped if the patent converted to NSR before the max dose, if the corrected QT interval increased by more than 35%, the QRS interval exceeded 120ms, or the patient’s heart rate dropped below 60BPM
- The length of stay between groups was not directly compared due to the fact that the shock-only group received a 30-minute placebo infusion followed by a 30-minute observation period to maintain blinding as this is what was done in the drug-shock group as well
- In patients who SBP dropped below 100mmHg, the infusion was interrupted for 15min and IV bolus of 250mL of 0.9% saline was administered. If the patient’s blood pressure returned to at least 100mmHg, the infusion was resumed, if not, the infusion was discontinued
- Patients allocated to the shock-only group received a similar weight-based infusion of 0.9% saline placebo over 30 minute before being randomized to one of the two pad placement strategies
- Pad positions for Protocol 2
- The sample size calculation for Protocol 1 was determined by a poll of investigators as there was no previous study to determine this number. A 90% power to detect an absolute difference of 10% between groups was predicted, assuming a control conversion rate of 85% for the shock-only group. A 10% difference may have been too ambitious. Even a 4% difference would still be significant (NNT = 25) but would require a much larger study
- Using either strategy resulted in almost 50% of patients being discharged home on anticoagulation. Depending on the patient’s insurance status and ability to follow up, this could be an issue. This evidenced by the fact that only 32 to 35% of patients in this trial had outpatient visits.
- The drug-shock group had more adverse events overall (most commonly transient hypotension), but the electrical cardioversion group had more hypoxia, requirement of airway maneuvers, and even one patient with cardiac arrest (that survived) due to lack of synchronization. Most of these can be attributed to the procedural sedation and not the cardioversion itself
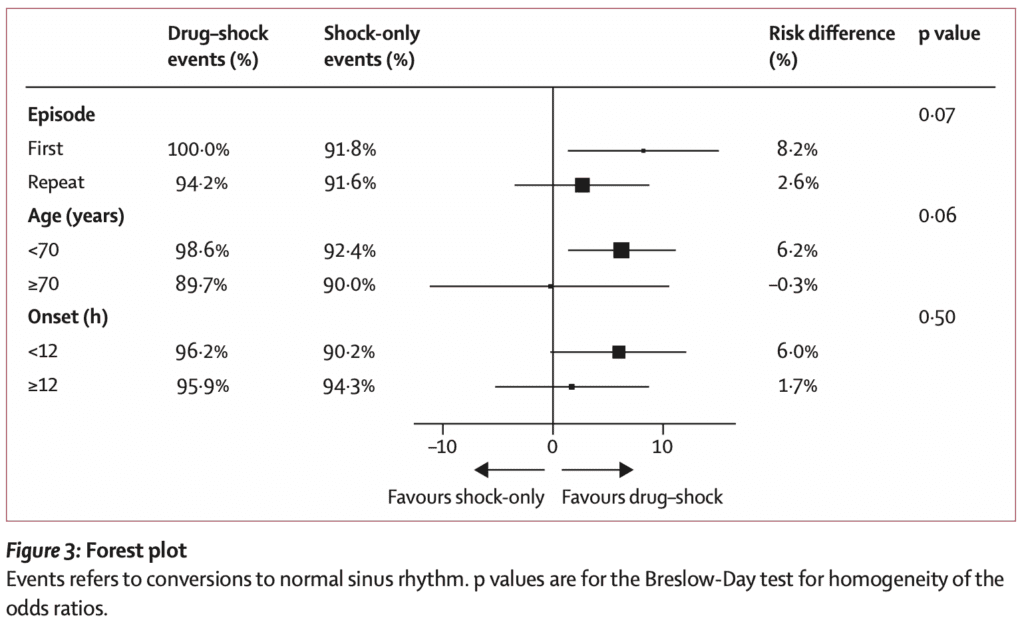
- A completely hypothesis generating result of the trial is that a drug-shock strategy was more effective for patients with a 1st episode of atrial fibrillation and for patients <70 years of age compared to other patients
- Discharge anticoagulation was determined by CHADS2 score ≥1 or age ≥65 years. The need for long-term oral anticoagulation was determined at follow up visit
Author Conclusion: “Both the drug-shock and shock-only strategies were highly effective, rapid, and safe in restoring sinus rhythm for patients in the emergency department with acute atrial fibrillation, avoiding the need for return to hospital. The drug infusion worked for about half of patients and avoided the resource intensive procedural sedation required for electrical cardioversion. We also found no significant difference between the anterolateral and anteroposterior pad positions for electrical cardioversion. Immediate rhythm control for patients in the emergency department with acute atrial fibrillation leads to excellent outcomes.”
Clinical Take Home Point: Both the drug-shock and shock-only strategies led to similar conversion rates and rates of discharge home. Length of stay was similar between groups; however this doesn’t reflect real-world application where a shock first approach would not get a 30 minute infusion of placebo for the purpose of blinding. Ultimately either approach is fine based on provider comfort, patient preference and departmental considerations.
References:
- Stiell IG et al. Electrical Versus Pharmacological Cardioversion for Emergency Department Patients with Acute Atrial Fibrillation (RAFF2): A Partial Factorial Randomised Trial. Lancet 2020. PMID: 32007169
For More Thoughts on This Topic Checkout:
- REBEL EM: AFib – Wait-and-See or Early Cardioversion to Obtain Normal Sinus Rhythm?
- REBEL EM: The BEST AF Trial – What is the Optimal Energy Selection for Cardioversion in Patients with Afib?
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)


The post RAFF2: Electrical vs Pharmacological Cardioversion for ED Patients with Acute Atrial Fibrillation appeared first on REBEL EM - Emergency Medicine Blog.