
 Background: Baloxavir (trade name Xofluza) was approved for the treatment of acute, uncomplicated influenza in patients > 12 years of age in October 2018. However, high-quality data has been underwhelming at best for its efficacy in treatment. Back in November of 2018, REBEL EM concluded:
Background: Baloxavir (trade name Xofluza) was approved for the treatment of acute, uncomplicated influenza in patients > 12 years of age in October 2018. However, high-quality data has been underwhelming at best for its efficacy in treatment. Back in November of 2018, REBEL EM concluded:
Clinical Take Home Point: Consistent with every other study on anti-viral medications for influenza, baloxavir appears to decrease duration of symptoms, especially in patients treated within 24 hours of symptoms, BUT a massive exclusion list, cost of the medication, increased resistance after initiation, results only applicable to H3N2 (88% of patients with flu), no comparison to standard care (i.e. symptom based therapy), pharma sponsored study, and no patient oriented outcomes, it is hard to make an argument for the use of baloxivir in patients with confirmed influenza. This trial should be a reminder as to why an industry funded trial, without full release of data, and cherry picked endpoints should not be used to change practice.
Continued research on effective anti-influenza drugs is critically important particularly with the potential for a “double pandemic” in the coming months. While treatment results are modest at best, baloxavir has potential as a prophylactic medication as well.
REBEL Cast Episode 86 – Baloxavir for Influenza Prophylaxis
Article: Ikematsu H et al. Baloxavir Marboxil for Prophylaxis Against Influenza in Household Contacts. NEJM 2020: 383(4): 309-20. PMID: 3260124
Clinical Question: Does a single dose of baloxavir to asymptomatic, close household contacts reduce the development of clinical influenza in this group in comparison to placebo?
Population: Household contacts who had no influenza symptoms (including fever) and lived in the same household as the index patient (positive rapid influenza test) for at least 48 hours before enrollment. Women of child-bearing age were included if they were using a highly effective contraception method.
Outcomes:
- Primary: Development of laboratory-confirmed clinical influenza (RT-PCR positivity for influenza virus RNA and the presence of both fever and at least one respiratory symptom of moderate or greater severity during the period from day 1 to day 10). Modified intention-to-treat analysis
-
Secondary:
- RT-PCR confirmed illness: RT-PCR confirmed infection + fever OR one influenza symptom
- RT-PCR confirmed influenza regardless of fever and symptoms
- Safety endpoints: clinical adverse events and abnormal laboratory values
Intervention: Single, weight-based (< 80 kg; 40 mg baloxavir > 80 kg; 80 mg baloxavir) oral dose of baloxavir
Control: Matching placebo
Design: Multicenter, double-blind, randomized, placebo-controlled trial in Japan
Excluded:
- Diagnosed with influenza during the 2018-2019 season
- Presence of other household contacts (aside from the index patient) with influenza symptoms
- Immunocompromised including steroids, immunosuppressants or HIV infection
- Prior use of an influenza, anti-viral in the last 30 days
- Allergy to baloxavir
- Severe underlying disease
- Women who were pregnant or lactating
- Any condition or circumstance that the investigator thought would compromise safety of the participant
Primary Results
-
-
Index Patients
- N = 545
- < 12 years old: 73.6%
- 95.6% with Influenza A (roughly 50% H1N1, 50% H3N2)
- All index patients treated with anti-viral medication (52.7% received baloxavir)
- 31.2% had influenza vaccination within previous 6 mo
-
Household Contacts
-
Number of subjects
- N = 752 randomized
- N = 749 analyzed in modified intention to treat
-
Subject age range
- < 12 years of age: 19%
- > 65 years of age: 3.1%
- 72.5% of patients received the study drug w/in 24 hours of onset of illness in the index patient
-
Number of subjects
-
Influenza vaccination within last 6 months
- Baloxavir group: 29.4%
- Placebo group: 30.7%
-
Index Patients
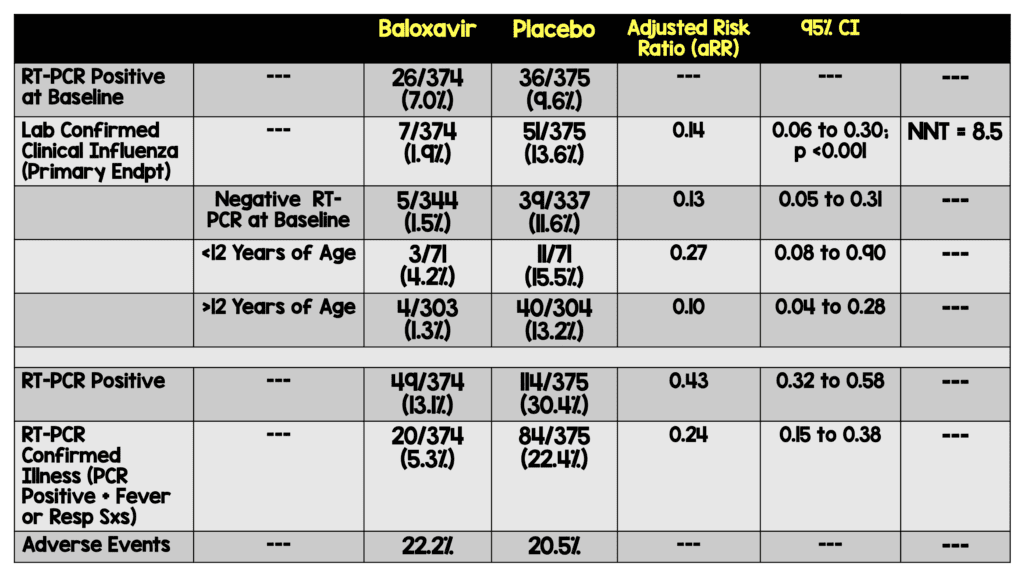
Critical Findings:
Strengths:
- Study asks a clinically relevant, patient centered question
- Patients’ demographics and baseline characteristics were well-balanced
- Study included a fair number (~ 19%) of patients < 12 years of age
- NP swabs were obtained at least at 3 points – prior to study drug, at 5 days and at 11 days (additional NP swabs were obtained if the patient developed fever and moderate to severe symptoms)
- Symptom assessors (self or guardian) were blinded to treatment arm
- Adverse events were about the same between groups and only one severe adverse outcome (typical psychosis) was seen (in the placebo group)
Limitations:
- Unclear if there was consecutive enrollment of contacts of index patients
- Symptom rating (i.e. moderate symptoms) was assessed either by self-evaluation (> 12 years of age) or by the participants guardian (< 12 years of age) and was subjective which may introduce bias.
- Exclusion criteria allowed for investigator subjectivity in enrollment which may bias results
- All index patients treated with antivirals
- Patients with significant illness and pregnant women were excluded
- Follow up samples of influenza were not obtained from index patients to ascertain the frequency of viral mutation after baloxavir administration
Discussion
- The study was designed by the manufacturer of baloxavir. Data was compiled by the sponsor and analyzed by a statistician employed by the sponsor.
- All index patients were treated with antivirals which is not standard practice in many areas. This may limit generalizability of the study results
- The study almost exclusively looked at influenza A (H1N1 and H3N2) and the results can only be applied to outbreaks of this influenza type
- The exclusion of patients with significant illness is unfortunate as this group may stand to benefit the most from prophylaxis
-
Roughly 30% of household contacts were immunized to influenza in the prior 6 months.
- We are not given subject level data to know if immunization status affected development of lab confirmed clinical influenza
- Unclear if baloxavir would perform as well in populations with higher immunization rates or if it would perform better in areas with lower vaccination rates
- Future research should look at the utility of this approach in other settings like schools, hospitals etc.
- Use of baloxavir led to an increased rate of mutations in the polymerase acidic protein (PA) endonuclease. This is important because these mutations make virus less susceptible to baloxavir and in some cases prolonged viral shedding (similar findings seen in study of baloxavir for treatment of those with influenza)
Authors Conclusions:
“Single-dose baloxavir showed significant postexposure prophylactic efficacy in preventing influenza in household contacts of patients with influenza.”
Our Conclusions: In this study, prophylactic, single-dose baloxavir appears to reduce the rate of lab confirmed clinical influenza in close household contacts of patients with confirmed clinical influenza type A who are taking antiviral medications.
Potential to Impact Current Practice: Single-dose baloxavir may be a useful prophylactic medication to prevent additional clinical infections in close household contacts. Based on this data, we only have an established benefit when the index patient has influenza A (the 2020 influenza season appears to be dominated by influenza B). The role of baloxavir for prophylaxis in those who are immunized as well as in those with significant comorbid disease is unknown.
For More on This Topic Checkout:
- REBEL EM: Baloxavir (Xofluza), a New Influenza Anti-Viral Medication is FDA Approved But, Does it Work?
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post REBEL Cast Ep86: Baloxavir for Influenza Prophylaxis appeared first on REBEL EM - Emergency Medicine Blog.