
 Airway Pressure Release Ventilation (APRV) is a mode of ventilation that allows spontaneous breathing throughout the ventilation cycle. It is a time-cycled mode of ventilation between two levels of positive airway pressure with the main time on the high level and a shorter period of time during the expiratory release to facilitate ventilation. This may not be a mode of ventilation many ED physicians are comfortable and have experience with and in this podcast Frank Lodeserto, MD reviews how to setup, titrate, and wean patients on this mode of ventilation.
Airway Pressure Release Ventilation (APRV) is a mode of ventilation that allows spontaneous breathing throughout the ventilation cycle. It is a time-cycled mode of ventilation between two levels of positive airway pressure with the main time on the high level and a shorter period of time during the expiratory release to facilitate ventilation. This may not be a mode of ventilation many ED physicians are comfortable and have experience with and in this podcast Frank Lodeserto, MD reviews how to setup, titrate, and wean patients on this mode of ventilation.
REBEL Crit Cast Episode 3.0 – Airway Pressure Release Ventilation (APRV) Made Simple
Click here for Direct Download of Podcast
How it Works
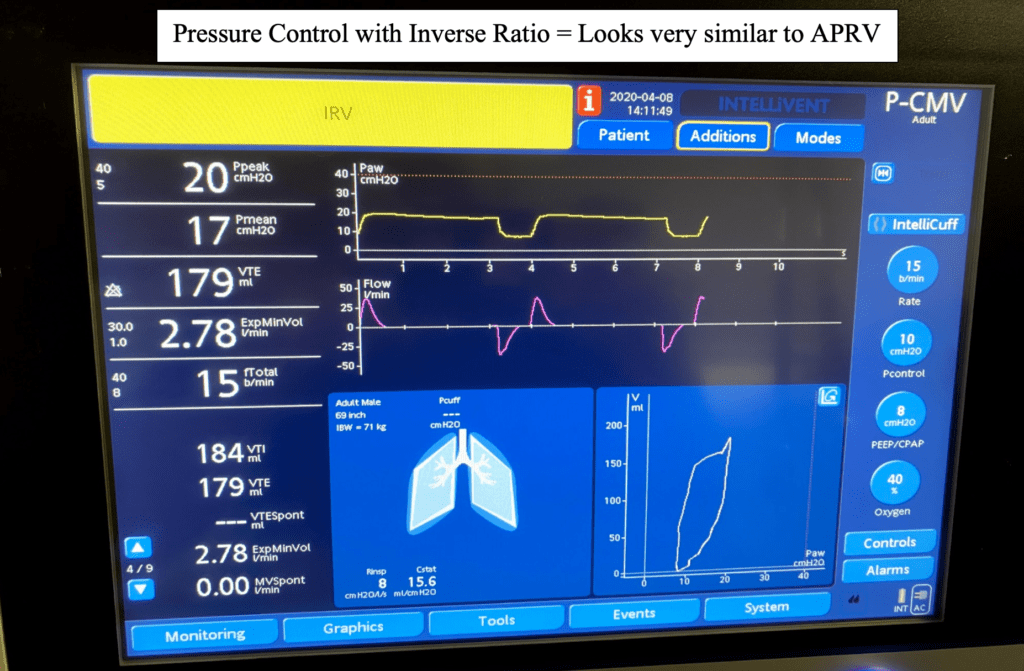
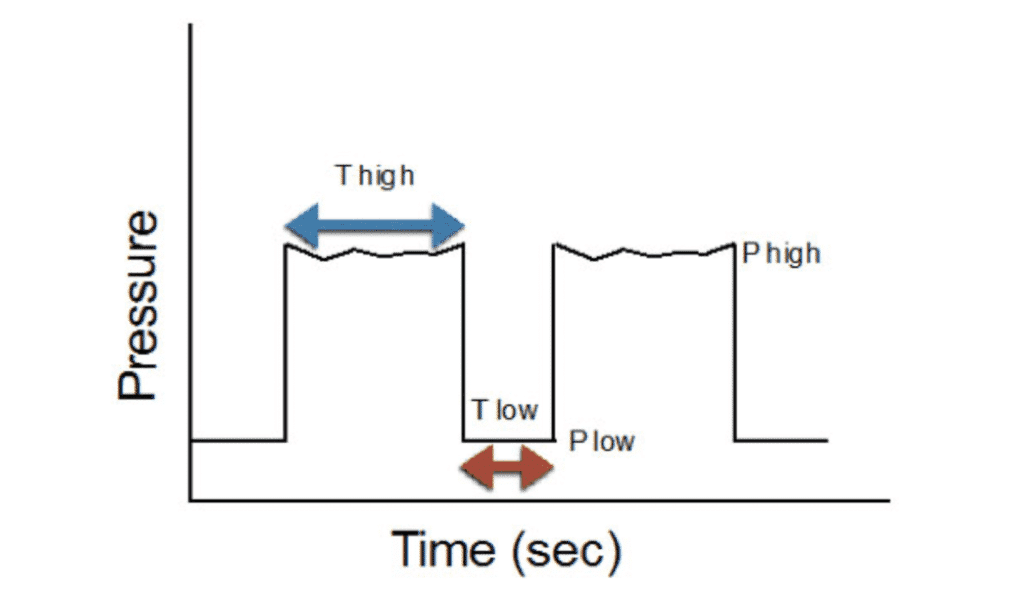
Airway Pressure Release Ventilation (APRV) is essentially 2 levels of CPAP. There is a high CPAP pressure known as the Phigh, and that pressure is held for a longer than usual time known as the Thigh. After this time ends there is a release where the pressure is allowed to drop to a lower pressure known as the Plow. This pressure release is usually very brief, and this time is known as the Tlow. Essential this mode is also very similar to Pressure Control (PC) with an inverse ratio (Long inspiratory time and short expiratory time) as shown below. PC is triggered (trigger = determines when breath is delivered), time cycled (cycle = causes ventilator to switch from inspiration to exhalation), and pressure limited (limit = maximal value achieved during inspiration). Just like PC, APRV is also triggered by time, time cycled, and pressure limited. APRV like Pressure Control, also delivers a set pressure and your tidal volume will vary based on you patient’s compliance. The difference is that APRV has an open dynamic expiratory valve that allows for spontaneous respirations both during the Phigh (inspiratory phase) and Plow phases (expiratory phase).
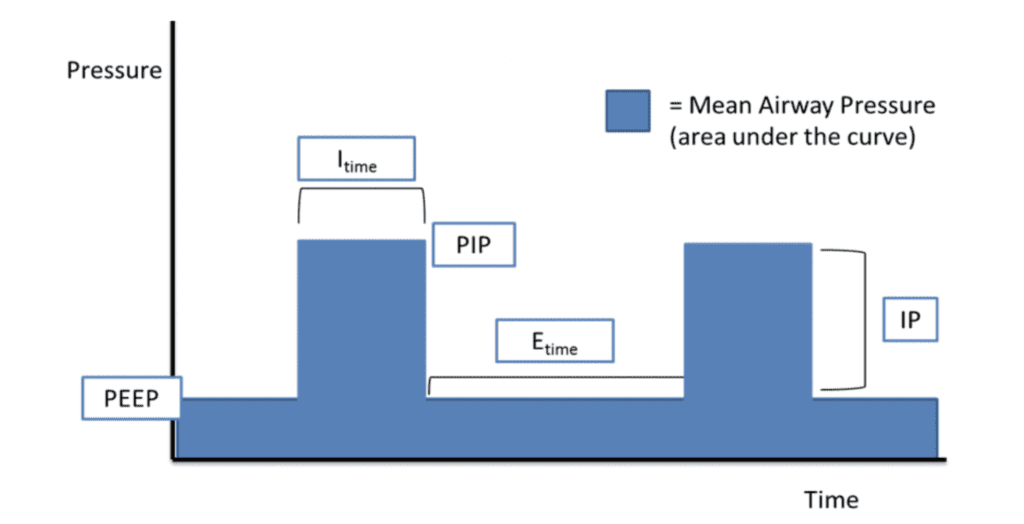
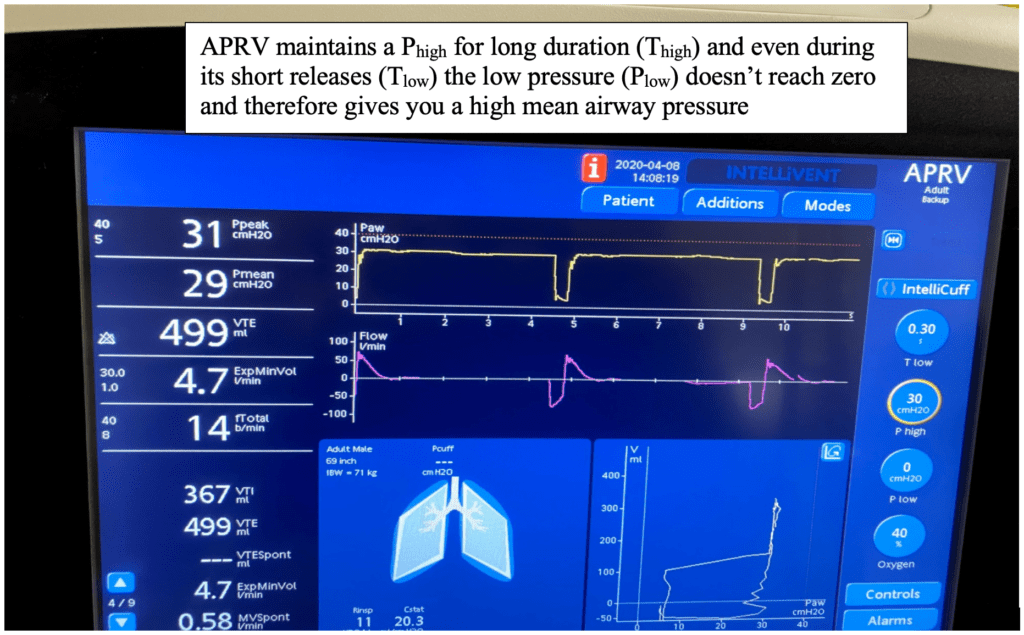
APRV utilizes an open lung strategy where the Phigh is sustained over a long duration (Thigh) to recruit and maintain recruitment of atelecotatic alveoli. It is effective in oxygenation because it can deliver a high mean airway pressure (MAP). We often don’t think of mean airway pressures, but this is the most important determinant of oxygenation. We often say that PEEP and Fi02 are the major determinants of oxygenation and this is true as we spend majority of our inspiratory cycle in expiration. We spend 1/3 of inspiratory cycle at the higher peak inspiratory pressure (PIP) and 2/3 of our time (longer in obstructive lung disease) in expiration. So the average pressure in our airways is determined mostly by our PEEP. In APRV however, we sustain this very high pressure for a long period of time increasing our mean airway pressure (MAP). The diagram below shows a conventional mechanical ventilation pressure graphic. As you can see, you only stay at this high inspiratory pressure for a shorter period of time compared to your expiratory pressure which is maintained twice as long. This is why you often hear people say that PEEP is one of the most important parameters to control oxygenation.
 (Image from Kevin Kuo, MD – Link is HERE)
(Image from Kevin Kuo, MD – Link is HERE)
Uses/Cautions:
- Can be used safely in patients with acute lung injury, acute respiratory distress syndrome (ARDS), and profound atelectasis. Avoid in patients with obstructive lung disease (Asthma, COPD).
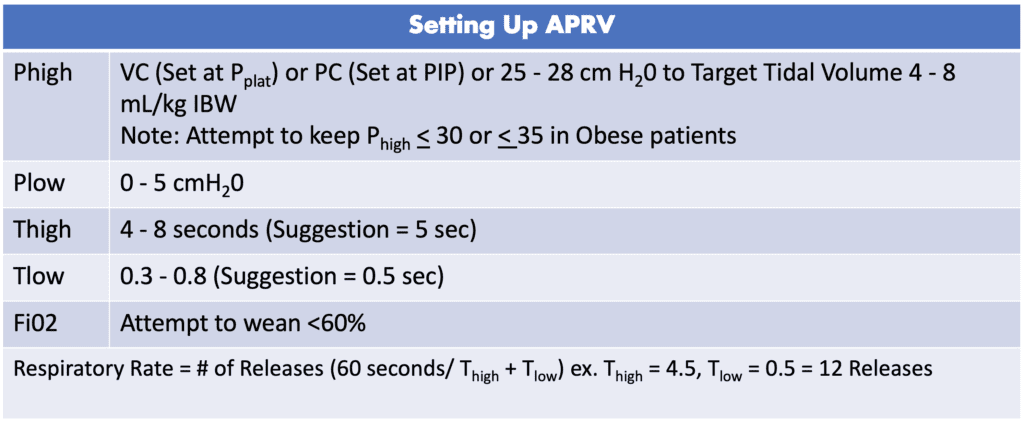
Setting up APRV:
[embedyt] https://www.youtube.com/watch?v=saVw9_OcViQ[/embedyt]
APRV-TCAV (Time Controlled Adaptive Ventilation) from EMCrit Website [Link is HERE]
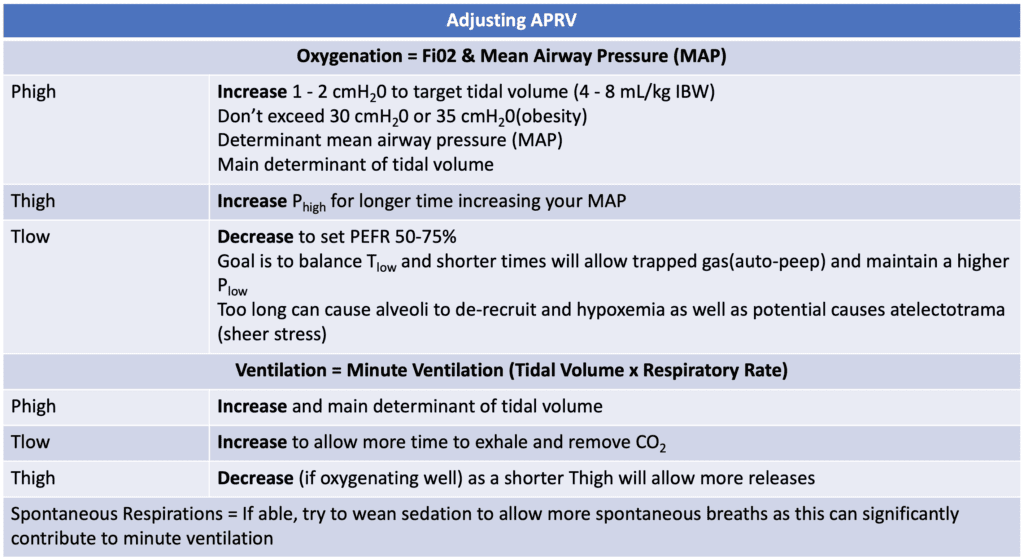
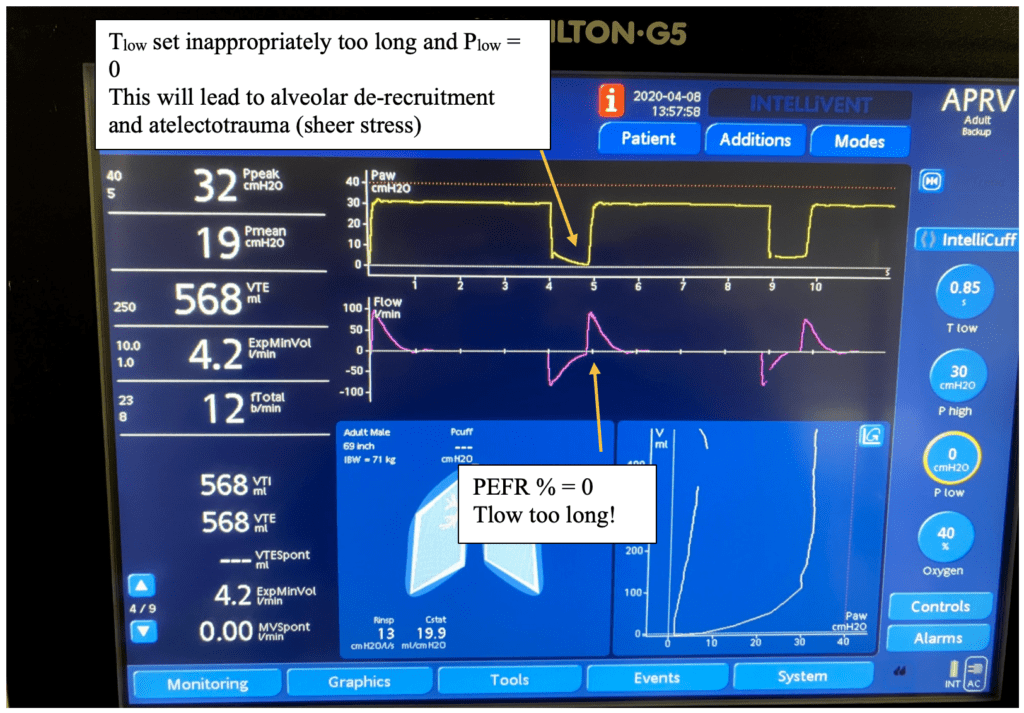
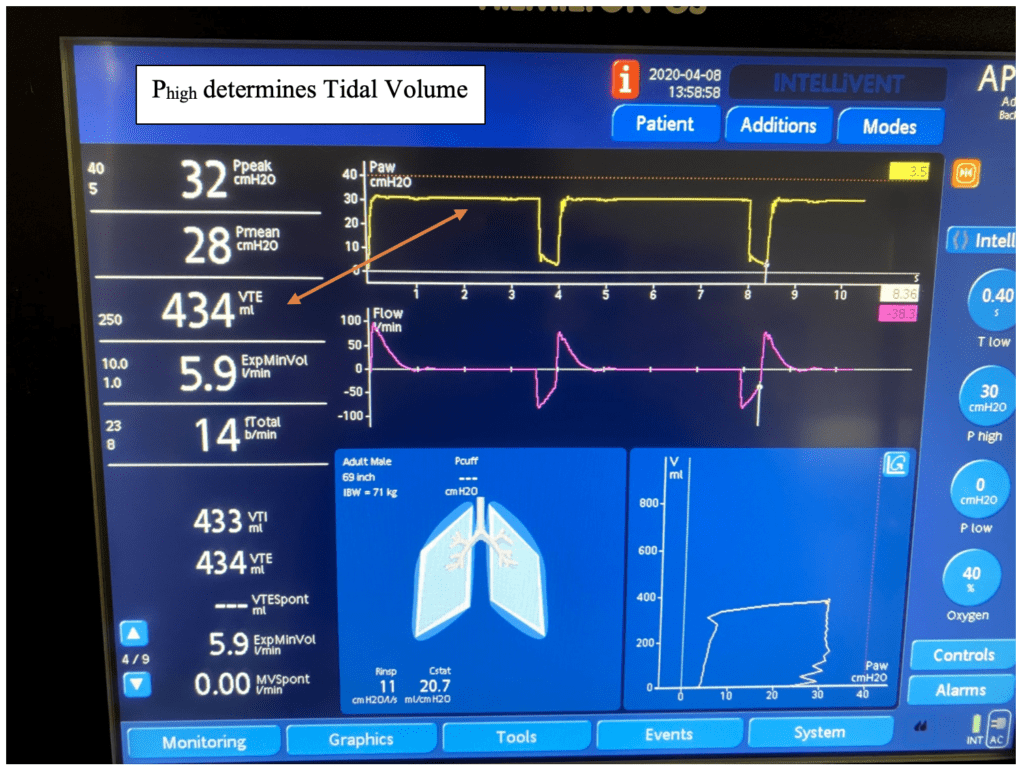
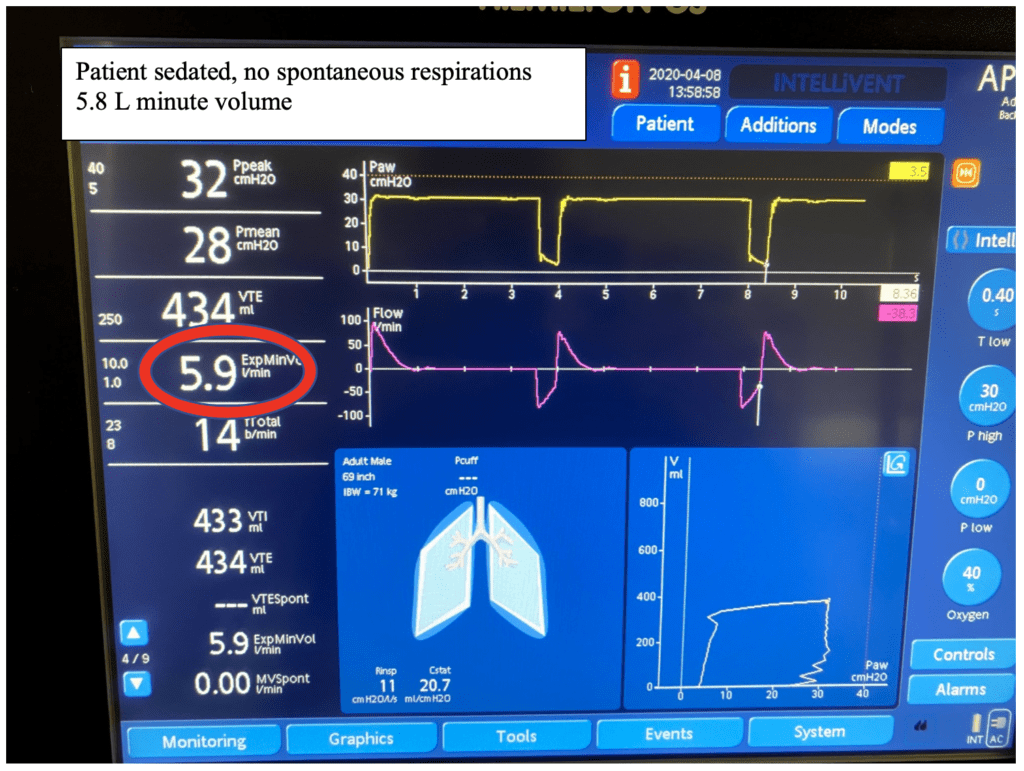
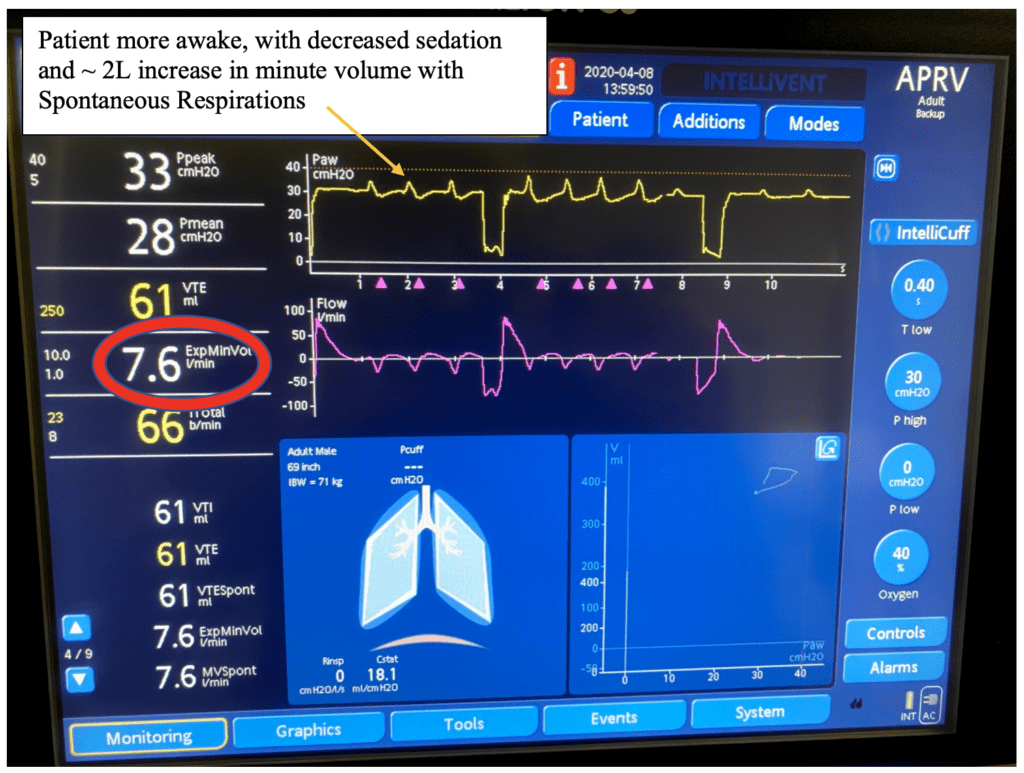
Adjusting APRV: Oxygenation & Ventilation
APRV Weaning:
- Goal: Fi02 < 50%, patient awakening with spontaneously breathing, and lung injury resolving.
- Start to decrease Phigh 1 – 2 cm H20 (DROP) and simultaneously increase Thigh 0.5 – 1 seconds (STRETCH). You dont need to change the Plow or Tlow. Increasing your Thigh will decrease the number of releases, so it’s important that your patient is awake and spontaneous breathing to help ventilate.
- Continue to “drop & stretch” every 2 – 4 hours as tolerated by patients: stop if patient has increased work of breathing, tachypnea and /or desaturation, as they may have de-recruited (and developed atelectasis) with weaning
- When the Phigh ~10 cmH20 and Thigh ~ 10 – 12 seconds, the patient is appropriate to consider switching to pressure support with PEEP in preparation for liberation from mechanical ventilation
Special Thanks to Joshua Vanhouten RT-ACCS
References:
- Zhou Y et al. Early Application of Airway Pressure Release Ventilation may Reduce the Duration of Mechanical Ventilation in Acute Respiratory Distress Syndrome. Intensive Care Medicine 2017. PMID:28936695
- Habashi NM et al. Other Approaches to Open-Lung Ventilation: Airway Pressure Release Ventilation. Crit Care Med 2005. PMID:15753733
For More Thoughts on This Topic Checkout:
- PulmCrit: IBCC Chapter – Guide to APRV for COVID-19
- EMCrit: COVID19 Respiratory Rescue and Ventilatory Optimization – Airway Pressure Release Ventilation (APRV) Time-Controlled Adaptive Ventilation
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post REBEL Crit Cast Ep3.0: Airway Pressure Release Ventilation (APRV) Made Simple appeared first on REBEL EM - Emergency Medicine Blog.