
 The subject of this ECG of the Week is a 47 y/o hispanic female with a past medical history of type 2 diabetes mellitus, hypertension, hyperlipidemia, and morbid obesity with a chief complaint of weakness. Per the patient she cleans houses for a living and for the past 2 weeks she gets weak and short of breath earlier in the day while cleaning houses. She used to be able to clean all day without issues, but for the past 2 weeks this has been getting less and less. No chest pain, vomiting, diaphoresis, or syncope. She has never had anything like this before. She comes to the ER today because this is her only day off. She has not had any symptoms today.
The subject of this ECG of the Week is a 47 y/o hispanic female with a past medical history of type 2 diabetes mellitus, hypertension, hyperlipidemia, and morbid obesity with a chief complaint of weakness. Per the patient she cleans houses for a living and for the past 2 weeks she gets weak and short of breath earlier in the day while cleaning houses. She used to be able to clean all day without issues, but for the past 2 weeks this has been getting less and less. No chest pain, vomiting, diaphoresis, or syncope. She has never had anything like this before. She comes to the ER today because this is her only day off. She has not had any symptoms today.
BP 156/94 HR 68 RR 14 O2 sat 100% on RA Temp 98.7
ECG from triage is shown…
Before reading on, try to come up with your own interpretation of this ECG before moving on to the final impression
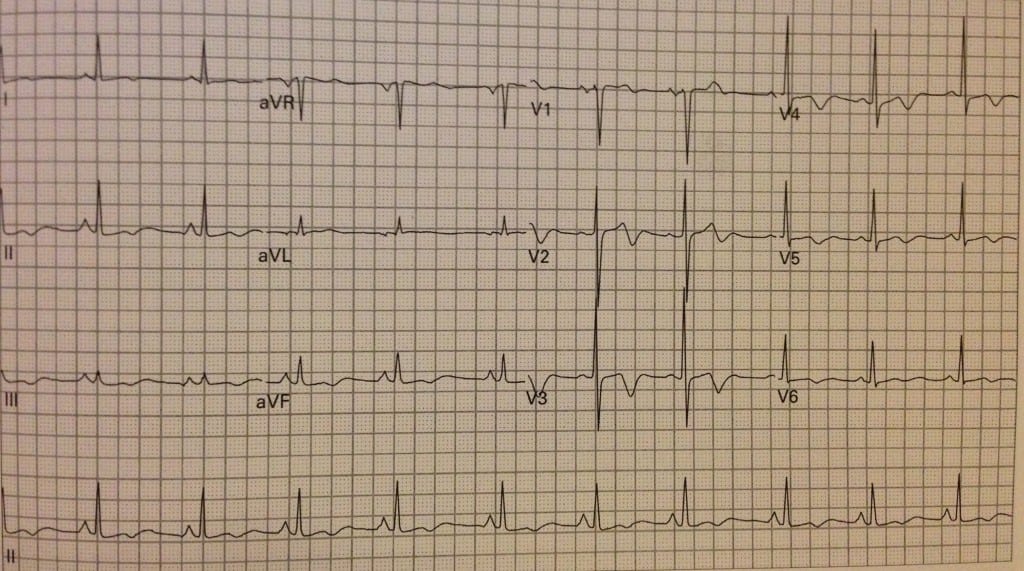
- Rate: Ventricular rate 60 bpm
- Rhythm: sinus
- Axis: normal axis
- QRS: narrow
- ST/T Waves: biphasic t-waves in precordial leads, no Q waves, and good R wave progression
- Final ECG Interpretation: Biphasic t-waves in leads V2 – V6 (Concerning for proximal LAD critical stenosis = Wellens’ Syndrome)
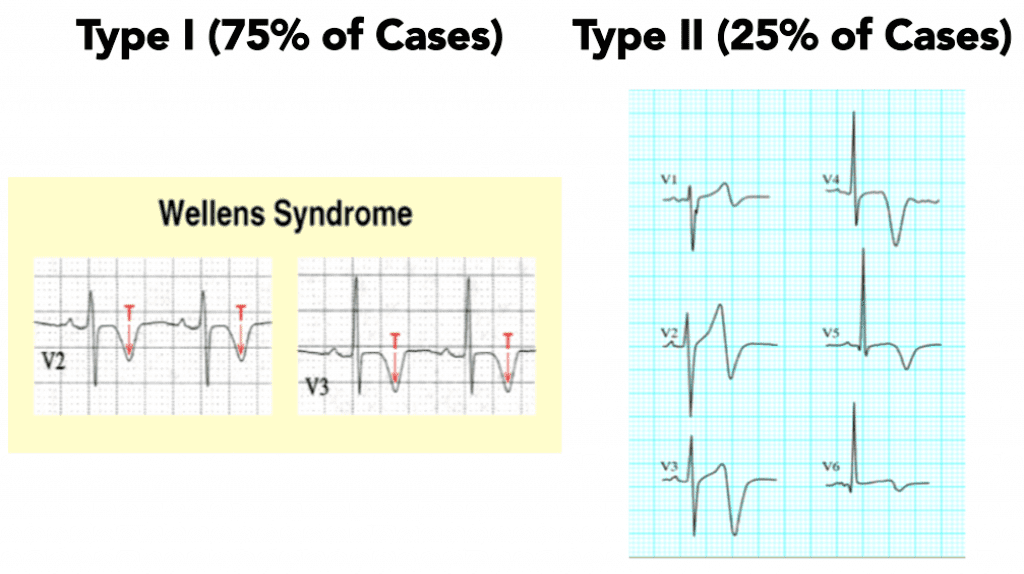
This is a case of Wellens’ Syndrome. Wellens’ is a pre-infarction stage of coronary artery disease and has some specific criteria for its diagnosis:
- History of angina + t-wave inversion or biphasic t-waves in V2 – V4
- Normal or minimally elevated cardiac biomarkers
- No pathologic precordial q waves or loss of precordial r wave progression
There are 2 types of Wellens’ syndrome: Type 1 and Type 2:
 The teaching that stress testing should be avoided in patients with Wellens’ Syndrome is based on CASE REPORTS (Best level evidence). The thought is increasing cardiac demand with a highly stenosed left anterior descending may lead to a large anterior myocardial infarction. Therefore these patients should receive early cardiac catheterization without stress testing.
The teaching that stress testing should be avoided in patients with Wellens’ Syndrome is based on CASE REPORTS (Best level evidence). The thought is increasing cardiac demand with a highly stenosed left anterior descending may lead to a large anterior myocardial infarction. Therefore these patients should receive early cardiac catheterization without stress testing.
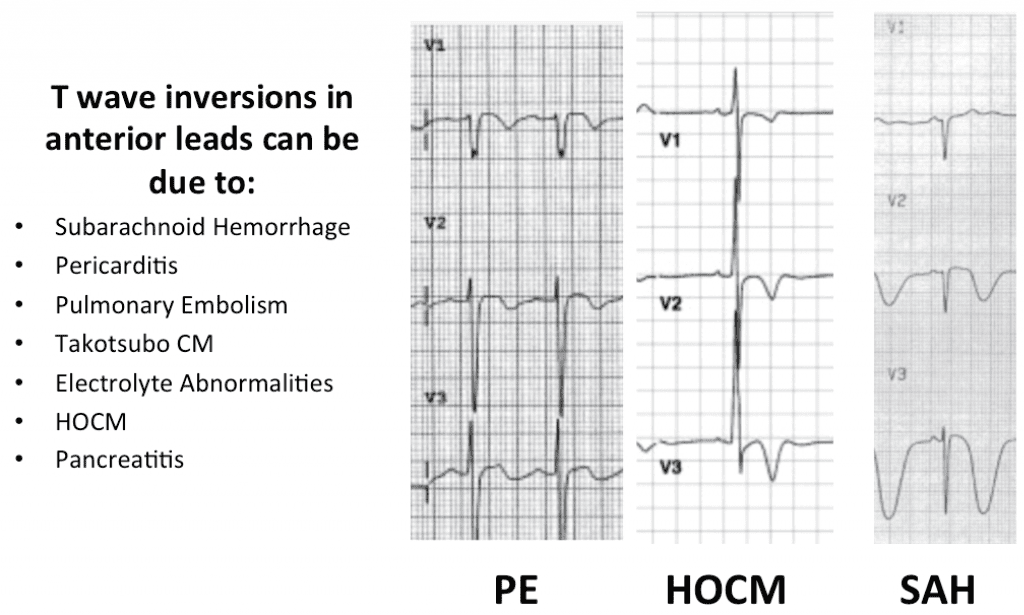
Finally, history is important. Just because a patient has t-wave inversions or biphasic t-waves on an ECG in the anterior leads, does not mean the patient has Wellens’ syndrome. Below are some examples of other pathologies that could cause similar t-wave abnormalities in the anterior leads.
 Case Conclusion: The cardiac catheterization report showed a 99% proximal LAD lesion consistent with biphasic t-waves seen in the V2 – V4 distribution.
Case Conclusion: The cardiac catheterization report showed a 99% proximal LAD lesion consistent with biphasic t-waves seen in the V2 – V4 distribution.
The post REBEL ECG of the Week #3 appeared first on REBEL EM - Emergency Medicine Blog.