
 Obstructive Physiology: Setting up the ventilator for a patient with severe obstructive physiology like asthma or COPD is almost a completely opposite strategy compared to the patient with severe metabolic acidosis. They both have problems with ventilation (removal of carbon dioxide), but for the patient with obstructive disease it takes a very long time to expire due to inflammation and bronchoconstriction. Instead of setting a high respiratory rate to blow off more CO2 like our severe metabolic acidosis patient, here, you want to set a low respiratory rate to give your patient time to empty more effectively.
Obstructive Physiology: Setting up the ventilator for a patient with severe obstructive physiology like asthma or COPD is almost a completely opposite strategy compared to the patient with severe metabolic acidosis. They both have problems with ventilation (removal of carbon dioxide), but for the patient with obstructive disease it takes a very long time to expire due to inflammation and bronchoconstriction. Instead of setting a high respiratory rate to blow off more CO2 like our severe metabolic acidosis patient, here, you want to set a low respiratory rate to give your patient time to empty more effectively.
Keys to setting up a ventilator in severe obstructive disease:
1.Don’t forget the ventilator is a supportive measure, so continue to treat your patients severe obstructive disease: analgesia & sedation, neuromuscular blockade, bronchodilators, steroids, Magnesium…etc.
2. Choose a mode that delivers volume breaths: Volume Assist/Control is a good option here for several reasons but there is no data to support one mode compared to others. Set your target tidal volumes no higher than 8 mL/kg based on ideal body weight (6-8mL/kg).
You can set your ventilator up in a pressure mode as well, but there is a reason I choose modes with volume breaths rather than pressure. Recall modes that deliver pressure breaths will deliver a pre-set pressure and not a set volume. Patients with severe obstructive disease will have high upper airway resistance, and therefore high PIP, but usually a low PPlat. The pressure will need be set very high to overcome upper airway resistance and the patient will likely not get adequate tidal volumes. Even if pressures are set very high, bronchospasm can worsen and you may have to increase pressures even more to deliver adequate tidal volumes. Most of your pressure will just be used to overcome the upper airway resistance and the patient may hardly get any delivered tidal volumes. Bronchospasm can also improve and then you will have to quickly lower the pressure to avoid too large a tidal volume.
So I simply place these patient in a volume mode and set my tidal volume between 6-8 mL/kg based on ideal body weight. I’ll discuss keeping tidal volumes in this range later, meaning 6 mL/kg, but in these patients I will often have to go to 8 mL/kg as you are limited on how you can clear CO2 given you are forced to keep the respiratory rate low due to their long expiratory phase.
Some of you may be thinking, why not give more than 8 mL/kg if you are limited by the slow rate and long expiratory phase. Tidal volumes greater than 8 mL/kg (10-12mL/kg) can lead to volutrauma (a form of ventilator induced lung injury (VILI) caused by delivering too large a tidal volume). Also, the more tidal volume you deliver to a patient with obstructive disease, the longer it will take that volume to be expired.
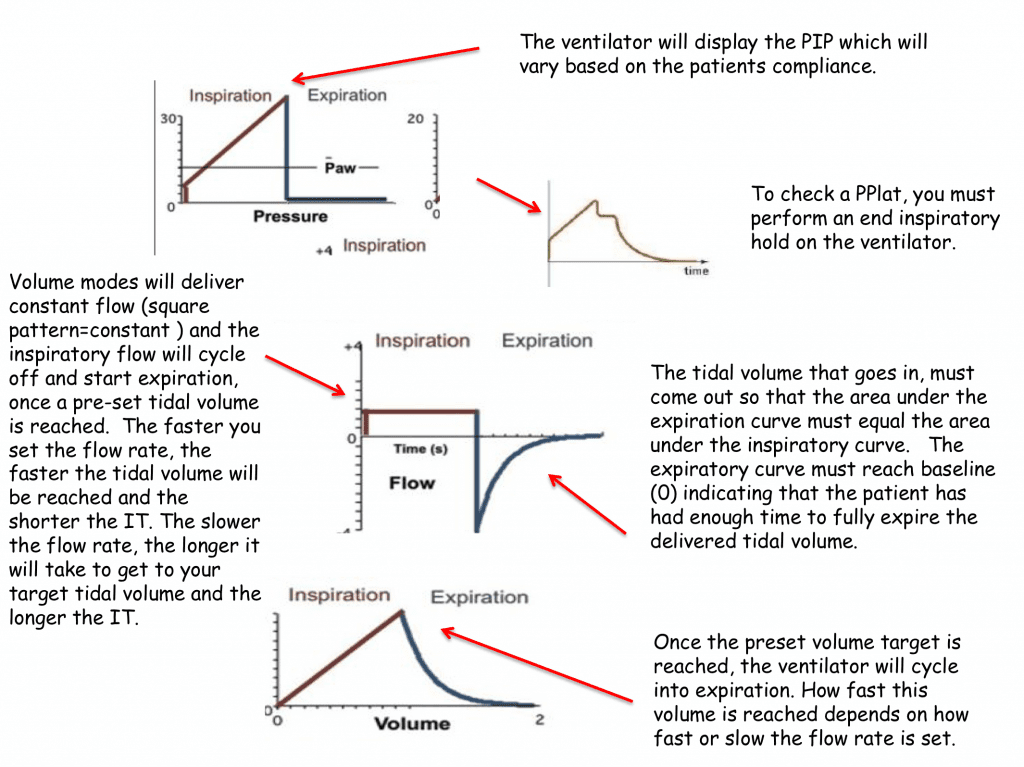
Figure 3: Normal Volume Mode Waveforms: Pressure vs. Time, Flow vs. Time, and Pressure vs. Time
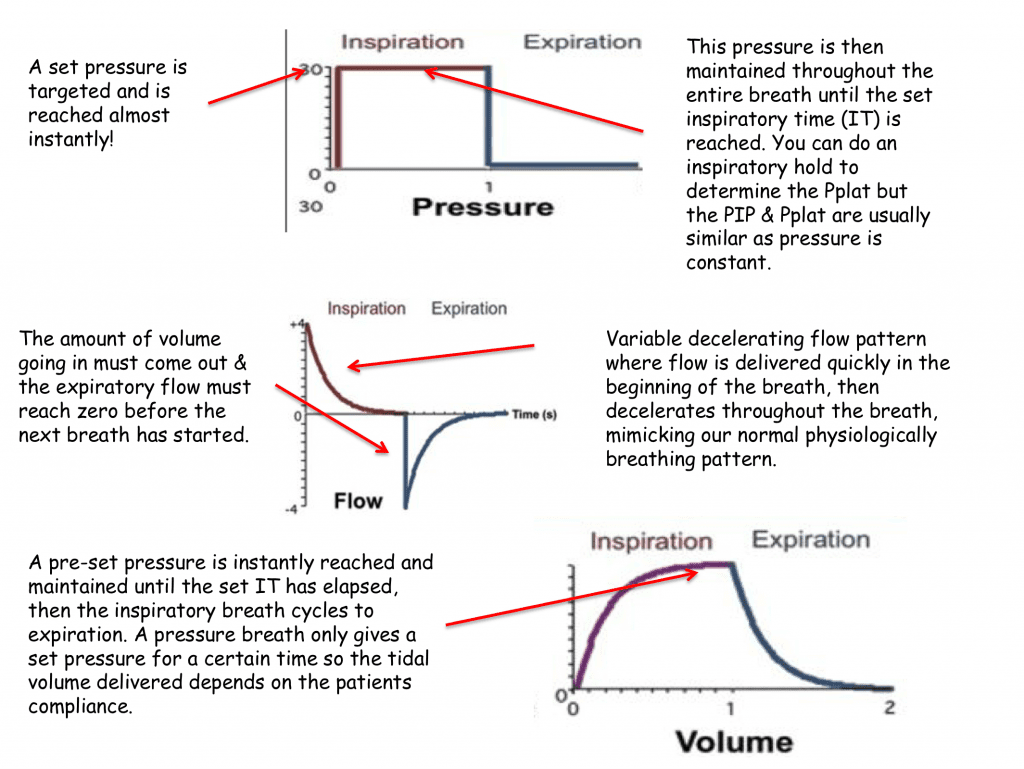
Figure 4: Normal Pressure Mode Waveforms: Pressure vs. Time, Flow vs. Time, Volume vs. Time
Please pay close attention to the waveform graphics above, particularly the flow vs. time waveform and notice how the expiratory flow returns to baseline indicating that your patient has fully exhaled and ready for their next breath. If this doesn’t happen (see figure 5 below) then the patient will may develop auto-peep due to dynamic hyperinflation.
What goes into the lungs must come out of the lungs, and if it doesn’t, then this volume will remain in the alveoli prior to the next breath being delivered. If this continues, then small amounts of volume will remain in the alveoli, breath after breath. This volume can get larger and larger and lead to elevated intra-thoracic pressure known as auto-peep.
3.Set your respiratory rate low and make sure your expiratory flow is reaching baseline prior to the next breath being delivered to avoid auto-peep.
After you intubate your patient and choose your initial ventilator settings take a look at the flow vs. time waveform to assure your patient has fully expired prior to the next breath being delivered. Check their flow vs time waveform initially and keep assessing this over time. Patients with obstructive physiology may not fully empty their alveolar volume to resting functional residual volume, a phenomenon known as dynamic hyperinflation. As a result of dynamic hyperinflation or inadequate emptying, patients can retain large amounts of volume in their alveoli, which can exert a pressure known as auto-peep. If this retained tidal volume or auto-peep becomes excessively large then it can cause severe complications such as pneumothorax or high intra-thoracic pressures which can decrease preload leading to hypotension and even cardiac arrest.
This is a nice spot to discuss the normal I:E (inspiration: expiration) ratio and breath cycle time. If you set the ventilator up to deliver 20 bpm, then this would give your patient 3 seconds to inspire and expire (breath cycle time would be 3 seconds). During this 3-second period, some of this time is spent in inspiration and some in expiration. If your normal I:E ratio is 1:2 then your patient may have 1 second to inspire and 2 seconds to expire. Your inspiratory time would be 1 second and your expiratory time would be 2 seconds.
In severe asthma or COPD exacerbations the I:E ratio can be 1:3 – 1:5, so it may take 5x as long to expire as it would be to inspire! To deliver 20 bpm with an I:E ratio of 1:5, then your inspiratory time would have to be 0.5 seconds and allow 2.5 seconds to exhale. This seems like it would work, but 0.5 seconds to deliver a normal tidal volume may be too fast and it may take your patient more that 2.5 seconds to expire. I typically set the rate low 8-12 bpm & give your patient 5-7.5 second breath cycles to ensure adequate emptying.
Below is a flow vs. time waveform from a volume delivered breath (notice square or constant flow). Pay attention to the expiratory flow curve, the red line (normal) reaches the baseline prior to the next breathe being delivered. The blue line expiratory flow does not reach zero prior to the next breath being delivered. When this happens, air is trapped in the alveoli and this gas can build up pressure known as auto-peep which as we mentioned can have serious consequences.
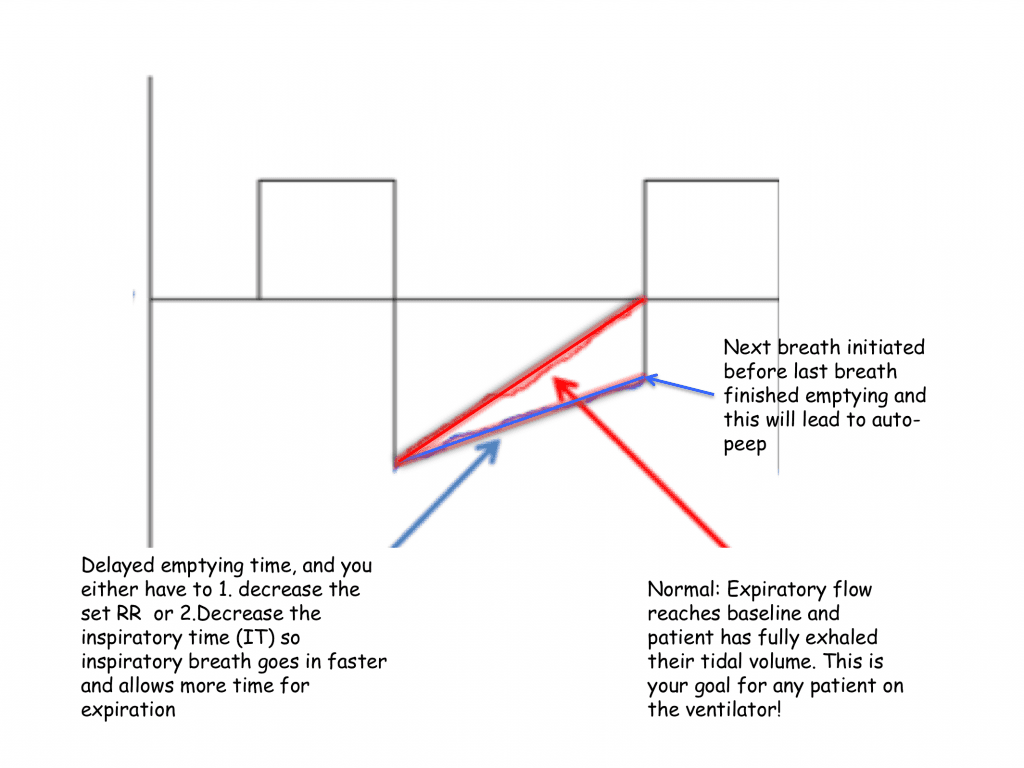
Figure 5: Flow vs Time Waveform displaying inadequate emptying and the development of auto-peep.
What should you do if this happens and you see the expiratory phase not reach baseline?
1.Reduce the respiratory rate first as this is usually the most effective intervention: Less breath cycles giving your patient more time to exhale
2.Increase your inspiratory flow rate (usually have to set the flow rate on a volume controlled ventilator mode). Normally a starting inspiratory flow rate may be 60-80 liters/minute. So if you set your inspiratory flow rate at 60 liters/minute that would deliver 1 liter/second to your patient. If you want to deliver a tidal volume of 500 mL’s then that breath would be delivered in 0.5 seconds. Increasing or decreasing your inspiratory flow rate will change how fast or slow you will be delivering your inspiratory volume. So in the obstructive patient, who you may want to allow more time to expire, then you can increase your inspiratory flow rate to deliver your tidal volume more quickly allowing more time to expire.
3.Some ventilator brands may ask you to change the I:E ratio. If you cannot adjust the flow rate by increasing the rate to deliver the tidal volume breath faster, then change your I:E ratio. By changing the I:E ratio you are accomplishing the same thing. Make the inspiratory time shorter and deliver the breath faster giving your patient more time to expire.
4.Check your PPlat frequently: Expect your PIP to be very high but frequently assess that your PPlat <30 mmHg and assure your staff that the PPLat is what the alveoli are seeing and not the PIP of 40-60 mm Hg.
I allow the ventilator to deliver the tidal volume breath understanding that the peak inspiratory pressure (PIP) may be very elevated as the ventilator attempts to overcome upper airway resistance. I then perform an end inspiratory pause to assess the plateau pressure with a goal of keeping the PPlat <30 mm Hg. Typically in severe obstructive disease, this pressure will be low unless they have combined parenchymal lung disease or the are developing auto-peep. Remember, the difference between PIP & PPLat is related to airway resistance, so you would expect a high PIP but a relatively low PPLat in severe obstructive disease (see Figure 6 below).
Please warn everyone that the PIP may be very high (40-60 mm Hg) and re-set your pressure ventilator alarm as this will constantly alarm due to high PIP, but explain to not worry as this pressure is not being transmitted to the alveoli and as long as the PPlat is less than 30 mm Hg.
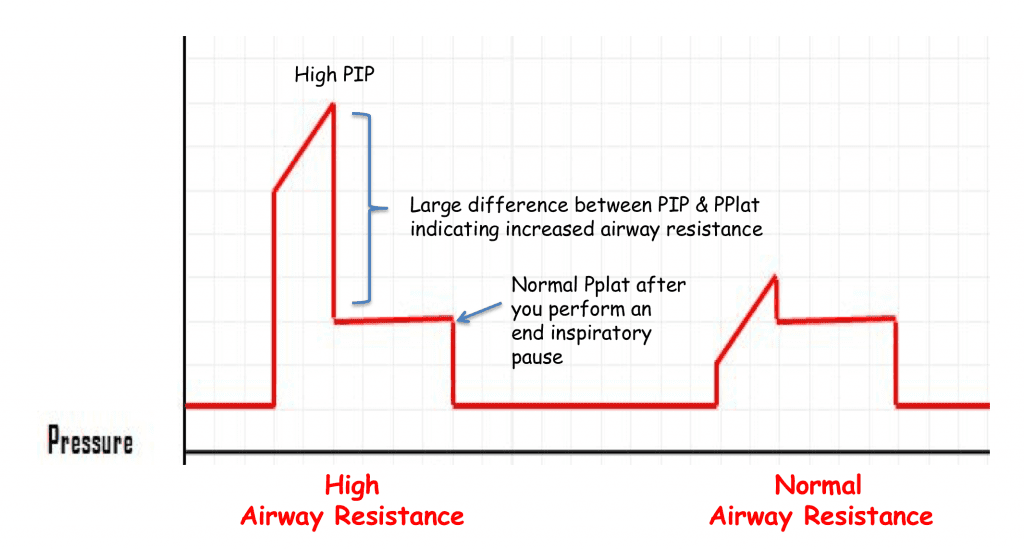
Figure 6
5.Set a low amount of PEEP, and a PEEP set to 5mm Hg to start should be perfect. I had been previously taught to use zero PEEP (known as ZEEP) as you did not want to further add to their existing auto-peep. However a small amount of PEEP may be beneficial to help keep open small-constricted bronchi that would normally collapse during expiration and worsen carbon dioxide removal.
6.Do not target a perfect blood gas and you can accept pH > 7.20, pCO2 <90 and goal 02 saturations 90-94%(more to be said about fi02 shortly). I mentioned earlier one of the goals of mechanical ventilation is adequate gas exchange, not perfect gas exchange. In very severe obstructive lung disease, you need to allow time for you therapies to work and the ventilator is just a supportive device to help oxygenate and ventilate.
When your patient is at the height of their disease process you may have to allow permissive (or in this case submissive hypercapnea). Allowing a respiratory acidosis will usually be well tolerated by most patients until your definitive therapies have time to work. If you try to make your blood gas perfect 7.4 pCO2 40 you may get into serious trouble. A pH > 7.2 with a pCO2 <90 may be the best you can get your patient safely, so don’t panic.
Just a note, permissive hypercapnea (or what I sometimes refer to as submissive hypercapnea = as there is nothing else you can do to safely improve ventilation, so you tolerate it or submit to the physiology) is often well tolerated. A few situations to be careful would be in (1) pregnancy as this may cause decrease in placental blood flow (2) Brain Injured patients with elevated intracranial pressure as high CO2 levels can increase intra-cerebral blood flow and elevate ICP due to increased blood flow (remember high CO2 levels and cause vasodilation of cerebral vasculature and low CO2 levels cause vasoconstriction to cerebral vasculature), and (3) severe pulmonary hypertension where a respiratory acidosis may cause increased pulmonary vascular resistance.
For More on This Topic Checkout:
- Frank Lodeserto at REBEL EM: Simplifying Mechanical Ventilation – Part I
- Frank Lodeserto at REBEL EM: Simplifying Mechanical Ventilation Part 2 – Goals of Mechanical Ventilation & Factors Controlling Oxygenation and Ventilation
- Frank Lodeserto at REBEL EM: Simplifying Mechanical Ventilation Part 3 – Severe Metabolic Acidosis
- Frank Lodeserto at REBEL EM: Simplifying Mechanical Ventilation Part 4 – Obstructive Physiology
- Frank Lodeserto at REBEL EM: Simplifying Mechanical Ventilation Part 5 – Refractory Hypoxemia & APRV
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
Support the Show by Paying & Claiming 1.5hrs (Parts 1 – 5) of CME/CEH by Clicking on the Logo Below
![]()
The post Simplifying Mechanical Ventilation – Part 4: Obstructive Physiology appeared first on REBEL EM - Emergency Medicine Blog.