
 Mechanical Ventilation is a modality commonly used in the critically ill, but many providers, may not have a strong understanding of the basics. Emergency Medicine and Critical Care Physicians need to have a firm grasp of the basic concepts of mechanical ventilation because without it, we can do serious harm to our patients. Airway management is not complete once the endotracheal tube is placed through the cords, and the proper selection of both the ventilator mode and initial settings is essential to ensure your patient has the best possible outcomes. You should not simply rely on the respiratory therapist to know your patients physiology. Clear communication with your therapist about the patient’s physiology and initial ventilator setting is crucial.
Mechanical Ventilation is a modality commonly used in the critically ill, but many providers, may not have a strong understanding of the basics. Emergency Medicine and Critical Care Physicians need to have a firm grasp of the basic concepts of mechanical ventilation because without it, we can do serious harm to our patients. Airway management is not complete once the endotracheal tube is placed through the cords, and the proper selection of both the ventilator mode and initial settings is essential to ensure your patient has the best possible outcomes. You should not simply rely on the respiratory therapist to know your patients physiology. Clear communication with your therapist about the patient’s physiology and initial ventilator setting is crucial.
Instead of going through all the various modes and learning them individually as most ventilator talks do, let’s try something different. Let’s first learn the 3 possible types of breaths your patient can receive on a ventilator and the 2 ways these breaths can be delivered. If you understand these concepts, then you can deconstruct almost any mode of mechanical ventilation and have a clearer understanding of how to use them. There are many modes that exist, but I suggest you learn a few, get to know them well, and when to apply each to your patient.
Mechanical Ventilator Breaths:
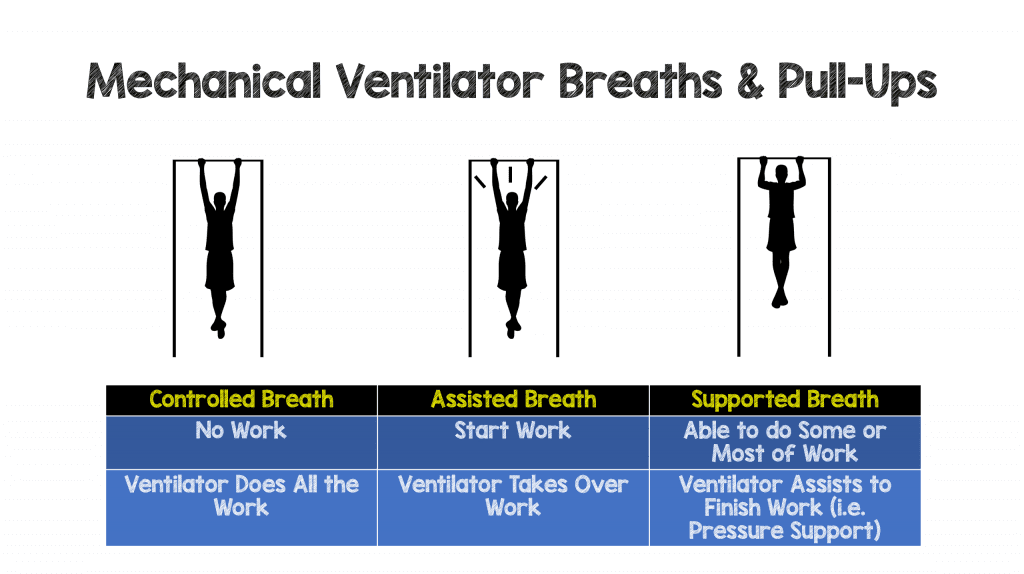
- Controlled Breaths: These breaths are completely “controlled” by the ventilator. A ventilator is purposely never set up in a mode with controlled breaths only. However, controlled breaths are delivered for safety at a set time interval if your patient is paralyzed or doesn’t have a respiratory drive (sedation, comatose, ect). Lets say your ventilator was set up with only controlled breaths at a respiratory rate (RR) of 10 breaths per minute (bpm). Then every 6 seconds a breath will be delivered to your patient no matter what. If your patient wants to take a breath at second 3, the ventilator will not allow this to happen. Essentially, with controlled breaths, your patient does absolutely no work and the ventilator does everything.
- Assisted Breaths: Just like hockey or basketball, if you pass the puck or the ball to your teammate and they score a basket or goal then you get an assist. The same concept is true with assisted breaths on a ventilator. Unlike the controlled breaths, which come at a set time interval, assist breaths will be delivered to your patient if they attempt to trigger a breath. If your patient attempts a breath (i.e. the pass the puck or ball) then the ventilator will sense this, and deliver a full mechanical breath (i.e. score goal or basket). For an assist breath, the patient must trigger the ventilator (sucking in on ETT and generate a change in pressure or flow), then the ventilator completely takes over and delivers a full breath.Lets say you place your patient on a mode called Assist/Control ventilation, then only 2 types of breaths can be delivered, controlled or assisted. If you set the RR at 12 bpm, then every 5 seconds the ventilator will deliver a preset breath if your patient doesn’t trigger a breath (paralyzed, sedated or comatose). These breaths will be all controlled breaths. However, if your patient is awake and initiating a breath sooner than every 4 seconds, these breaths will be assisted breaths. Essentially with an assist breath, your patient will initiate a breath, but the ventilator will take over and complete the work for the patient.
- Supported (Spontaneous) Breaths: These types of breaths are triggered by patient effort (like assisted breaths), but once triggered the ventilator will give you some support, but not full support like an assisted breath. I think of these breaths like supported pull-ups at the gym.
Control: You can only hang from the pull up bar, but are so weak you cant even initiate a pull up. Then you need a good friend to push you up till you get to the top of the bar.
Assisted: Here you can hang from the bar, and at least try to pull yourself up, but again your good friend sees your effort and helps you full get to the top of the bar.
Supported: Here you can start to pull up and maybe even get ¼ – ¾ up the bar but you need a little support or boost to complete the pull up.
 In a mode that only gives you supported breaths (Pressure Support or Volume Support) you have to ensure that the patient has an adequate respiratory rate (no RR is set on the ventilator) and has adequate respiratory effort, as your patient has to do work here to ensure an adequate tidal volume. In a Pressure support mode, all of your breaths are supported with some pressure. The most popular mode in pediatric critical care (not used much in adults) is SIMV + PS, and actually combines all three types of these breaths together as we will soon discuss.
In a mode that only gives you supported breaths (Pressure Support or Volume Support) you have to ensure that the patient has an adequate respiratory rate (no RR is set on the ventilator) and has adequate respiratory effort, as your patient has to do work here to ensure an adequate tidal volume. In a Pressure support mode, all of your breaths are supported with some pressure. The most popular mode in pediatric critical care (not used much in adults) is SIMV + PS, and actually combines all three types of these breaths together as we will soon discuss.
Breathe Delivery:
Volume Breaths: Just like it sounds, once the ventilator is triggered (time triggered controlled or patient triggered-assisted breath), the ventilator will deliver a preset tidal volume. In a volume mode, once the ventilator is triggered a preset tidal volume is given and once that set volume is achieved, the ventilator will cycle off into exhalation. During a volume delivered breath, you of course know the volume delivered to your patient, but what you don’t know is how much pressure it took for that breath to be delivered. This is a function of lung compliance (lung stretchiness). Compliance is simply the change in volume divided by the change in pressure (C=V/P).
A lung that is very stiff (Acute Respiratory Distress Syndrome), will have a low compliance and you would expect that it would take higher pressures to deliver that set tidal volume. If the lung has a high compliance (Emphysema), you would expect lower pressures to deliver that preset tidal volume.
On a volume mode (ex. Volume Assist-Control), you need to observe how much pressure it takes for that breath to be delivered. The pressure you should be most concerned about is the Plateau Pressure (PPlat), the pressure needed to distend the small airways and alveoli ( or the pressure needed to overcome the elastic forces of the lung ie alveoli and chest wall). High plateau pressures are reflective of problems with a patient’s lung compliance (The lungs are getting stiffer and the goal is to keep <30cmH20). This pressure will not be displayed on the ventilator, but can be achieved by performing an end-inspiratory hold maneuver (pauses the ventilator at the end of inspiration for 0.5-1 second).
The pressure that the ventilator will actually display for is the Peak Inspiratory Pressure (PIP). The PIP is the maximum pressure needed to deliver a breath during active inspiration. The PIP is the total of both resistive pressure (pressure to overcome endotracheal tube and the large proximal airways) as well as the elastic pressure of the lung (pressure to distend the small airways and the alveoli).
Summary of PIP and Plateau Pressures:
Imagine that your lungs are a balloon, and you are a ventilator trying to fill that balloon up. When you first start blowing up a balloon, it takes a lot of pressure to overcome the resistive forces of that balloon and start airflow, but once you overcome this resistance, the pressure needed to continue to fill the balloon to its full volume decrease. The same is true when the ventilator starts to deliver a breath; it takes a high amount of pressure to overcome the resistive forces of the endotracheal tube and upper proximal airways. If you were to stop airflow once the balloon is at full volume and tie it off and allow the pressure to equilibrate, then that pressure would be equivalent to your PPlat. Plateau pressure is the pressure at the alveolar level and if it’s set too high is capable of causing injury (High Pressure = Barotrauma or High Distending Volume=Volutrauma). PPl at may also reflect the fact that your patient’s lung compliance is decreasing (lungs are getting stiffer and therefore more pressure is needed to distend alveoli). Normally the difference between your PIP and PPlat is usually <5 cmH20 (PIP always > PPlat).
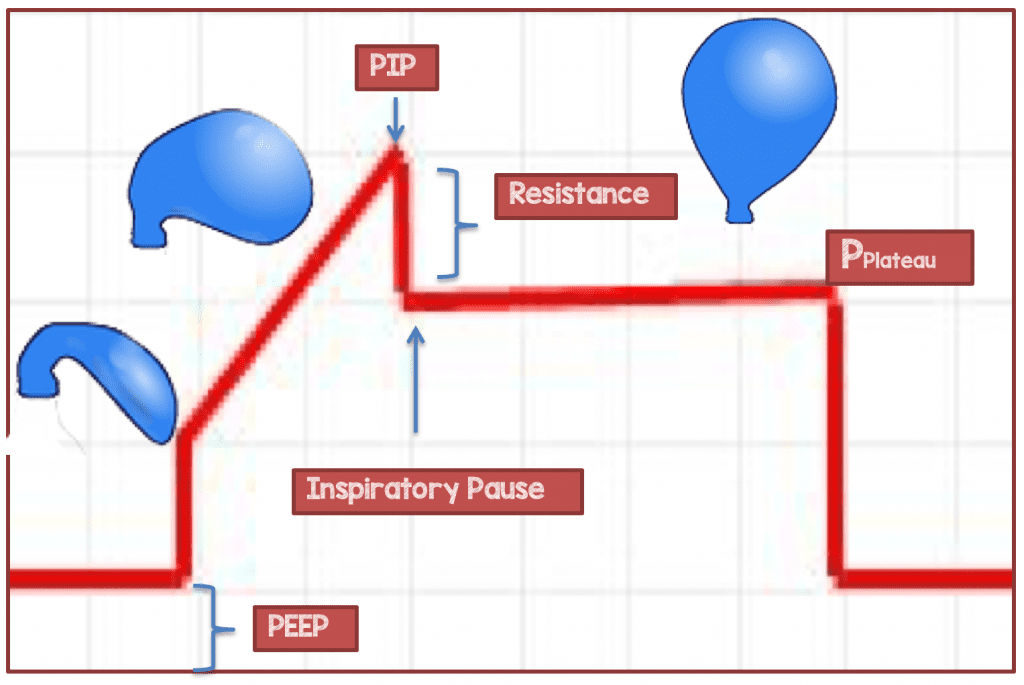
- Peak Inspiratory Pressure (PIP): Dynamic pressure needed to fully inflate the lung (Overcome resistive and elastic forces of the lung)
- Airway Resistance: PIP – Plateau Pressure (Normally <5cmH20 unless excessive airway resistance)
- Inspiratory Pause: Ventilator Maneuver to Measure Plateau Pressure
- Plateau Pressure (PPlat): Alveolar distending pressure (Static pressure which reflects lung compliance)
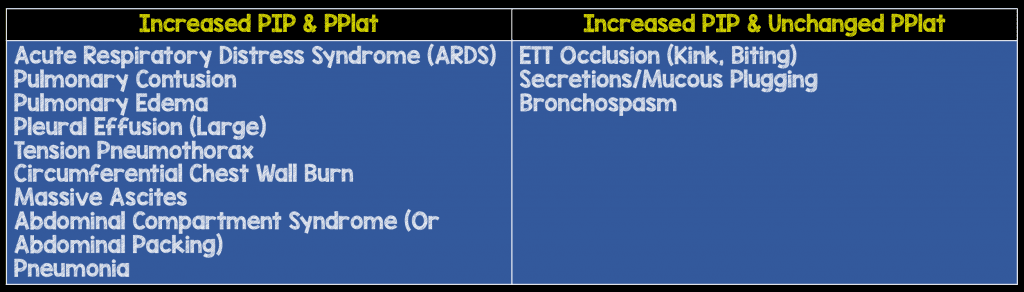
If your PIP and Plateau are both elevated then this indicates lung disease and decreased compliance of the lung, but if your PIP is elevated and your Plateau pressure is unchanged then this indicates increased airway resistance
Pressure Breaths: Again, just as the name implies, a preset pressure will be delivered to the patient once the ventilator is triggered (whether by time-pressure controlled breath or by patient effort-pressure assisted breath). In a pressure mode, the preset pressure is reached almost instantly and remains at that pressure for a set time (inspiratory time) and then cycles to exhalation once that time is reached.
So what tidal volume is your patient receiving with a pressure breath? With a pressure delivered breaths you have to ensure that your patient is getting an adequate tidal volume (>4cc/kg & < 8cc/kg IBW) by adjusting your ventilator pressures. It’s important to note that Ideal Body Weight (IBW) is based on your patient’s height, not on their actual weight. So, a 5-foot 150kg male should have the same tidal volume of a 5-foot 70 kg male. The volume that your patients will receive is going to be dependent on their lung compliance. A very stiff lung may require high pressures to deliver an adequate tidal volume and you may have to frequently adjust the pressure. If the patient’s compliance increases (less stiff) then you need to lower the pressure to ensure that the patient doesn’t get large tidal volumes. If your compliance is getting lower (stiffer lungs) then you may have to give higher pressures to ensure adequate tidal volumes.
If you have to constantly check a patient’s tidal volumes with pressures breaths then why use it? It’s because pressure breaths are believed to be physiologic and therefore more comfortable for your patient. We physiologically breathe with a decelerating flow pattern, where a large amount of gas rushes into our lungs very quickly then slows during the latter phase of inspiration. Pressure breaths mimic our normal flow pattern, where your set pressure is reached almost instantly causing a very large amount of gas to enter the lungs over a short period of time then slows down throughout inspiration. Toward the end, I will describe a mode that takes advantage of this decelerating flow pattern (more comfort) but targets a tidal volume, known as Pressure Regulated Volume Control (PRVC).
Modes:
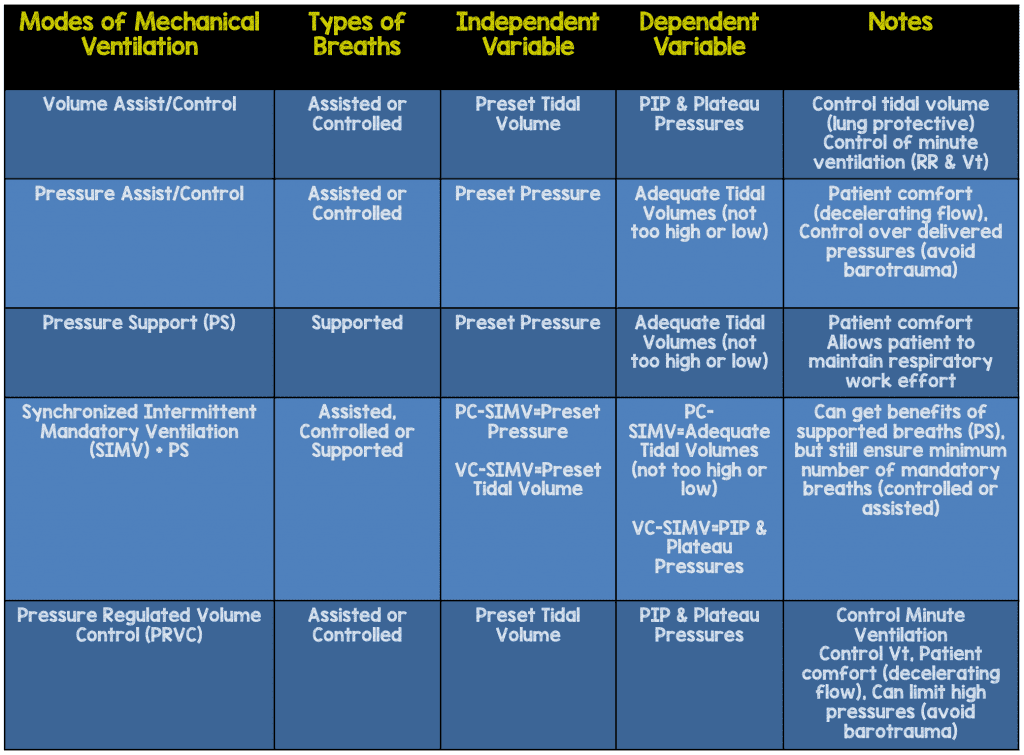
You now know many modes whether you realize it or not just by knowing the breath types (Controlled, Assisted, Supported) and how the breaths are delivered (Volume or Pressure).
Volume Assist Control
In this mode you need to set a respiratory rate and a tidal volume (Vt). You will also set a PEEP and Fi02 (but we will discuss this in another post). If you set the RR=12bpm and Vt=400cc (6cc/kg IBW) then every 5 seconds your patient will get a volume controlled breath at 400cc. If the patient is awake and triggering’s a breath faster than 12bpm, then these breaths will be volume-assisted breaths at 400cc. If your PIP is elevated remember to check your patients PPlat to ensure its less than 30cmH20.
Pressure Assist Control
In this mode you need to set a respiratory rate and a pressure. You will also set a PEEP and Fi02 (but we will discuss this in another post). If you set the RR=12bpm and Pressure = 15cmH20 (Set/Adjust Pressure to target 6cc/kg IBW) then every 5 seconds your patient will get a pressure breath at 15 mm Hg (remember to check their Vt). If the patient is awake and triggering’s a breath faster than 12bpm, then these breaths will be a pressure-assisted breath at 15cmH20.
Pressure Support
In this mode the patient will have to be able to both initiate the breath and have enough respiratory strength to take an adequate tidal volume. This mode is often used to decide if a patient can be extubated and used frequently in a spontaneous breathing trail (SBT). In a SBT, no RR is set and a minimal amount of PS (PS=5cmH20) is set and your assessing to see if your patient is comfortably breathing at a normal RR with adequate Vt (at least 4-6cc/kg) before extubating. If you choose to put a patient on pressure support, then just like pressure assist-control you have to adjust the pressure support to ensure that your patient is getting adequate tidal volumes (>4cc/kg & < 8cc/kg). A pressure supported breath will deliver that set pressure until the inspiratory flow decreases to a % of its peak flow (usually 25%) then the breath cycles into exhalation. You can terminate the breath sooner or later by adjusting the % of peak flow (40%-breath will cycle to exhalation sooner, 15%-the breath will cycle to exhalation later). PS differs from a pressure assist-control breath where the set pressure is delivered for a set time (inspiratory time). Pressure support can be added to other modes, as I will explain next.
Volume-SIMV (Synchronized Mandatory Ventilation) + PS:
With an understanding of all three types of breaths you will now be able to understand SIMV because it is capable of delivering all 3 types of breaths. In this mode you once again set the RR, Vt as well as fi02 and PEEP. If you set the RR=12 and the Vt=400cc, then every 5 seconds your patient will get a volume controlled breath at 400cc per breath if your patient does not have an adequate respiratory drive or a volume assisted breath if they are able to trigger. You will get 12 mandatory breaths (the RR you set=the number of mandatory breaths) and these will either be controlled, if patient makes no effort, or assisted, if they do trigger the ventilator at or near every 5th second. The ventilator will synchronize with the patient effort and give an assisted breath if the patient initiates their breath at or near every 5th second.
If your patient wants to breath in between those 5 seconds, then this breath will be a supported breath with pressure support. So with SIMV you will get a mandatory number of breaths (based on the set RR and will be either controlled or assisted), but additionally your patient has the ability to take supported breaths as well. This mode can also be set to be Pressure-SIMV + PS and the same concepts hold true, however instead of getting those mandatory breaths as volume controlled or volume assisted they will be pressure controlled or pressure assisted. SIMV is the mode we most commonly use in Pediatrics and in the Pediatric ICU. There are a few reasons for this, which I will explain, in another post.
Pressure Regulated Volume Control (PRVC): This mode is considered a pressure mode as the breaths given are pressure breaths with a decelerating inspiratory flow (more physiologic & comfortable), but targets a tidal volume so that you can ensure adequate tidal volumes as lung compliance changes. I often tell learners that a small therapist was shrunk and put inside the ventilator to assist the patient. Breaths can be controlled or assisted, but once triggered the mini therapist inside the ventilator calculates the patient’s lung compliance and delivers a set tidal volume, but does so at the lowest possible pressure. If compliance decreases, then more pressure is needed to achieve the set tidal volume. A safety alarm will alert providers (mini therapist calling for help). The pressure alarm is set usually set at 30-35cmH20 to avoid high pressures at the alveoli level known as barotrauma. The alarm usually sounds at 5cmH20 less than the alarm is set to, and warns providers that the pressure to achieve the tidal volume is getting higher (compliance decreasing). Once this high pressure is reached, then inspiration stops (no more tidal volume given) and the breath cycles to exhalation. PRVC can also be used in SIMV + PS which is commonly done in the PICU as well. This seems like the ultimate mode but it has some important disadvantages and not appropriate for some patients, which we will discuss in another post.
In the next post we will discuss how to choose your ventilator mode and initial settings based on your patients physiology
For More on this Topic Checkout:
- Frank Lodeserto at REBEL EM: Simplifying Mechanical Ventilation Part 2 – Goals of Mechanical Ventilation & Factors Controlling Oxygenation and Ventilation
- Frank Lodeserto at REBEL EM: Simplifying Mechanical Ventilation Part 3 – Severe Metabolic Acidosis
- Frank Lodeserto at REBEL EM: Simplifying Mechanical Ventilation Part 4 – Obstructive Physiology
- Frank Lodeserto at REBEL EM: Simplifying Mechanical Ventilation Part 5 – Refractory Hypoxemia & APRV
Post Peer Reviewed By: Salim R. Rezaie (Twitter: @srrezaie)
Support the Show by Paying & Claiming 1.5hrs (Parts 1 – 5) of CME/CEH by Clicking on the Logo Below
![]()
The post Simplifying Mechanical Ventilation – Part I: Types of Breaths appeared first on REBEL EM - Emergency Medicine Blog.