
 Background: In patients with compromised renal function, the use of intravascular iodinated contrast material is generally not given to avoid contrast induced nephropathy (CIN). Currently, there is no treatment for contrast-induced nephropathy, therefore the focus has been on prevention. Guidelines recommend prophylactic prehydration in the prevention of CIN in high risk patients. These recommendations are based on expert consensus and until now, there has not been a prospective randomized trial of IV hydration versus no hydration in high-risk patients.
Background: In patients with compromised renal function, the use of intravascular iodinated contrast material is generally not given to avoid contrast induced nephropathy (CIN). Currently, there is no treatment for contrast-induced nephropathy, therefore the focus has been on prevention. Guidelines recommend prophylactic prehydration in the prevention of CIN in high risk patients. These recommendations are based on expert consensus and until now, there has not been a prospective randomized trial of IV hydration versus no hydration in high-risk patients.
What They Did:
- Prospective, randomized, phase 3, parallel-group, open-label, non-inferiority trial
- High-risk patients (i.e.defined by an estimated glomerular filtration rate of 30 – 59 mL per min/1.73m2) who were undergoing an elective procedure requiring iodinated contrast material administration were randomly assigned to receive: IV 0.9% Normal Saline vs No IV Fluids
Hydration Protocols:
- Standard Protocol: IV 0.9% NaCL 3 – 4mL/kg per hr during 4hr before and 4hr after contrast administration
- Long Protocol: Intravenous 0.9% NaCl 1mL/kg per hr during 12hr before and 12hr after contrast administration
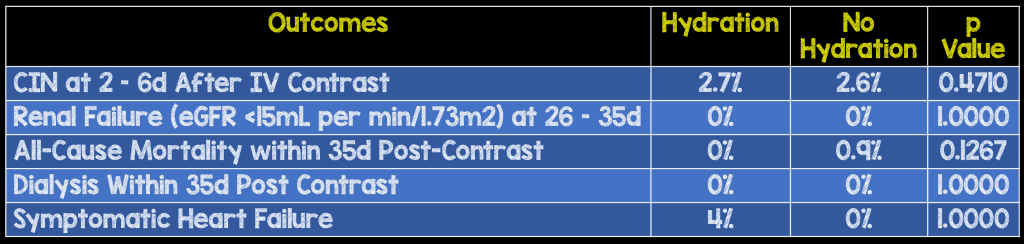
Outcomes:
- Primary: Incidence of Contrast-Induced Nephropathy – Defined as an increase in serum creatinine from baseline of more than 25% or 44umol/L within 2 – 6 days after contrast exposure
-
Secondary:
- Mean change in serum creatinine from baseline at 2 – 6 and 26 – 35days after contrast administration
- Major Adverse Events: All-Cause Mortality, Renal Replacement Therapy, Intensive Care Admission, and Sequelae of Fluid Administration
- Major Renal Adverse Events: Renal Failure (Defined as eGFR <15mL per min/1.73m2), renal decline with >10 eGFR units, renal decline to eGFR <30mL per min/1.73m2, or a combination of the latter two, at 26 – 35 days
- Major Fluid Administration Events: Symptomatic Heart Failure, Hypernatremia or Hyponatremia, and Supraventricular or Ventricular arrhythmias
- Cost-effectiveness of no prophylaxis compared with intravenous hydration
Inclusion:
- Estimated glomerular filtration rate (eGFR) between 45 – 59mL per min/1.73m2 combined with either diabetes, OR at least two predefined risk factors (age >75years, anemia defined as hematocrit <0.39 L/L for men and <0.36 L/L for women, Cardiovascular disease, Non-steroidal anti-inflammatory drug or diuretic nephrotoxic medication
- eGFR between 30 – 45 mL per min/1.73m2
- Multiple Myeloma
- Lymphoplasmacytic Lymphoma with small chain proteinuria
Exclusion:
- Inability to Obtain Informed Consent
- eGFR < 30 mL per min/1.73m2
- Renal Replacement Therapy
- Emergency Procedures
- Intensive Care Patients
- Known Inability to Plan Primary Endpoint Data Collection
- No Referral for Prophylactic Hydration
- Participation in Another Randomized Trial
- Isolation (Infection Control)
Results:
- >650 patients randomized
Strengths:
- Prospective, Randomized Clinical Trial
- Consecutive Patients
- Blinding of laboratory staff
- Randomization stratified to Preplanned Subgroup Analyses: Diabetes (yes vs no), eGFR (<45 vs ≥45 mL per min/1.73m2), contrast administration route (Intravenous vs Intra-arterial, and procedure type (diagnostic vs interventional)
- Baseline characteristics balanced between groups
- Data for serum creatinine level at days 2 – 6 was available for 91% of the 660 patients
Limitations:
- Single Center
- Sample size reduced during the study from 1300 to 600 patients, but most likely did not affect validity of study as non-inferiority margin of 2.1% was predefined
- Open-label design because masking of intervention was almost impossible
- Post contrast serum creatinine measurements not available for all patients, but baseline characteristics of patients were similar to patients included in the study
- Due to the paucity of placebo-controlled trials on the effectiveness of prophylactic hydration, setting a non-inferiority margin for contrast-induced nephropathy was difficult (Assumed incidence of CIN would be 2.4% and chose a non-inferiority margin of 2.1%)
Discussion:
- In this trial minimum volume, pre-warmed, low-osmolar, monomer, non—ionic, contrast material lopromide, at 300mg iodine per mL. were used, not high osmolar contrast media
- Mean total IV hydration volume given in the prehydration group was 1637mL and Mean volume of contrast material administered was 91mL
Author Conclusion: “We found no prophylaxis to be non-inferior and cost-saving in preventing contrast-induced nephropathy compared with intravenous hydration according to current clinical practice guidelines.”
Clinical Take Home Point: This is the first prospective, randomized clinical trial evaluating the effectiveness of intravenous prehydration to prevent CIN in high risk patients. With the low- and iso-osmolar contrast agents being used today, withholding prophylaxis for high risk patients with an eGFR >29 mL per min/1.73m2 may be feasible and cost saving, but this still warrants external validation prior to implementation.
References:
- Nijssen EC et al. Prophylactic Hydration to Protect Renal Function from Intravascular Iodinated Contrast material in Patients at High Risk of Contrast-Induced Nephropathy (AMACING): A Prospective, Randomised, Phase 3, Controlled, Open-Label, Non-Inferiority Trial. Lancet 2017; S0140 – 6736(17)30057 – 0. PMID: 28233565
For More Thoughts on This Topic Checkout:
- Richard Sinert at EMDocs: Nephropathy – Confounding Causation
- Celia Bradford at The Bottom Line: Prophylactic Hydration to Protect Renal Function from Intravascular Iodinated Contrast material in Patients at High Risk of Contrast-Induced Nephropathy
Post Peer Reviewed By: Scott Wieters (Twitter: EMedCoach)
The post The AMACING Trial: Prehydration to Prevent Contrast Induced Nephropathy (CIN)? appeared first on REBEL EM - Emergency Medicine Blog.