
 In the fall of 2014, while working overnight in the emergency department at a community hospital in NJ, a patient (let’s call him John) presented with ACE inhibitor angioedema. At first glance, his lips were swollen, but his tongue and oropharynx were unremarkable, and there were no signs of respiratory distress. I ordered an “anaphylaxis cocktail” and checked on him a few moments later.
In the fall of 2014, while working overnight in the emergency department at a community hospital in NJ, a patient (let’s call him John) presented with ACE inhibitor angioedema. At first glance, his lips were swollen, but his tongue and oropharynx were unremarkable, and there were no signs of respiratory distress. I ordered an “anaphylaxis cocktail” and checked on him a few moments later.
John’s condition deteriorated. His tongue, now swollen, protruded and forced his mouth open. He spoke in a muffled voice and drooled his oral secretions. I quickly phoned anesthesia for fiberoptic intubation. My heart sank when I was notified they were unavailable.
Sullenly, I pressed forward. When you’re expecting salvation from a consultant, moments requiring life-sustaining procedures can be paralyzing. You can be disabled by an inert sense that a hero is coming. When you’re the only physician available, the realization that no one is coming to the rescue can be very empowering. You are that hero!
I moved down my airway algorithm. First, I placed the video laryngoscope into John’s airway and could see only fleshy pink pleats of soft tissue and frothy viscous oral secretions. The limited space in the airway vanished, and John crashed rapidly. He desaturated to 60%, became cyanotic, and his eyes bulged from his skull. He choked and gasped violently for air. Then, he became bradycardic.
John was about to die. Next, I switched to his neck and fumbled nervously with the components of a cric kit. Then, I grabbed a #11 blade scalpel and made a sizeable vertical midline neck incision. I pierced his cricothyroid membrane and a turbulent audible whoosh erupted from John’s neck as air escaped. Blood pooled in the incision site and spattered the team as they watched. I placed my finger through the now patent cricothyroid membrane, followed by a bougie, then an endotracheal tube. The respiratory therapist connected John to the ventilator and the team and I waited anxiously as his vital signs normalized.
Cricothyroidotomy is a rare procedure I performed many times in simulation, but never on an actual patient in a life-and-death situation. Either by coincidence, luck, or divine intervention, I watched a video on finger-guided bougie-assisted cricothyroidotomy just days before. I felt clarity on the requisite steps and qualified to perform them. I was intensely focused and had no sense of worry, self, time, or personal needs. When we secured the tube and saved John’s life, I felt an overwhelming sense of euphoria. This is my most vivid experience in flow.
WHAT MAKES AN EMERGENCY MEDICINE DOCTOR HAPPY?
Autotelic is a term derived from the Greek words auto (self) and telos (goal). Autotelic activities are intrinsically motivating—the activity is the reward and it’s done for the pursuit of happiness.
I often participate in interviews with prospective emergency medicine residents—each candidate, highly motivated and highly accomplished. But, many have a difficult time articulating precisely why they want to be an emergency medicine physician. Through self-reflection, I discovered I too share this burden.
I’ve practiced emergency medicine for 13 years and often feel if I couldn’t perform my duties, I would do something entirely outside of medicine. It seems taboo to say, “I love being in life-and-death situations,” where what you do matters instantly. Why emergency medicine? Perhaps emergency medicine is autotelic. The answer quite possibly is flow.
Mihaly Csikszentmihaly, a psychologist and leading expert in flow states, found that the happiest people had the most flow states and structured their lives to deliver the most flow states. Author Steven Kotler writes in The Rise of Superman: “flow is the hallmark of high performance, but in situations where the slightest error could be fatal, then perfection is the only choice—and flow is the only guarantee of perfection.”
Kotler, however, refers to extreme sports athletes and conceives their rich environment guarantees access to the flow state. He juxtaposes the massive progression of extreme sports to marginal improvements in traditional sports. He proposes that flow is to the extreme sports athlete what the yellow sun is to Superman, the source of power.
The rich environment in the emergency department and fertile soil provided in life-and-death situations also grants access to flow. There is an abundance of literature on flow in psychology but virtually none in the practice of medicine. However, I contend the practice of emergency medicine provides the most flow states of all specialties. We in emergency medicine may be flow junkies.
WHAT IS FLOW?
Athletes refer to it as “the zone.” It’s also been called “mystical experience” and “peak experience.” For thousands of years, many religions and cultures have described similar states. Csikszentmihaly describes flow as “An automatic, effortless, yet highly focused state of consciousness.” He further explains: “You are in an ecstatic state to such a point that you feel as though you almost don’t exist.”
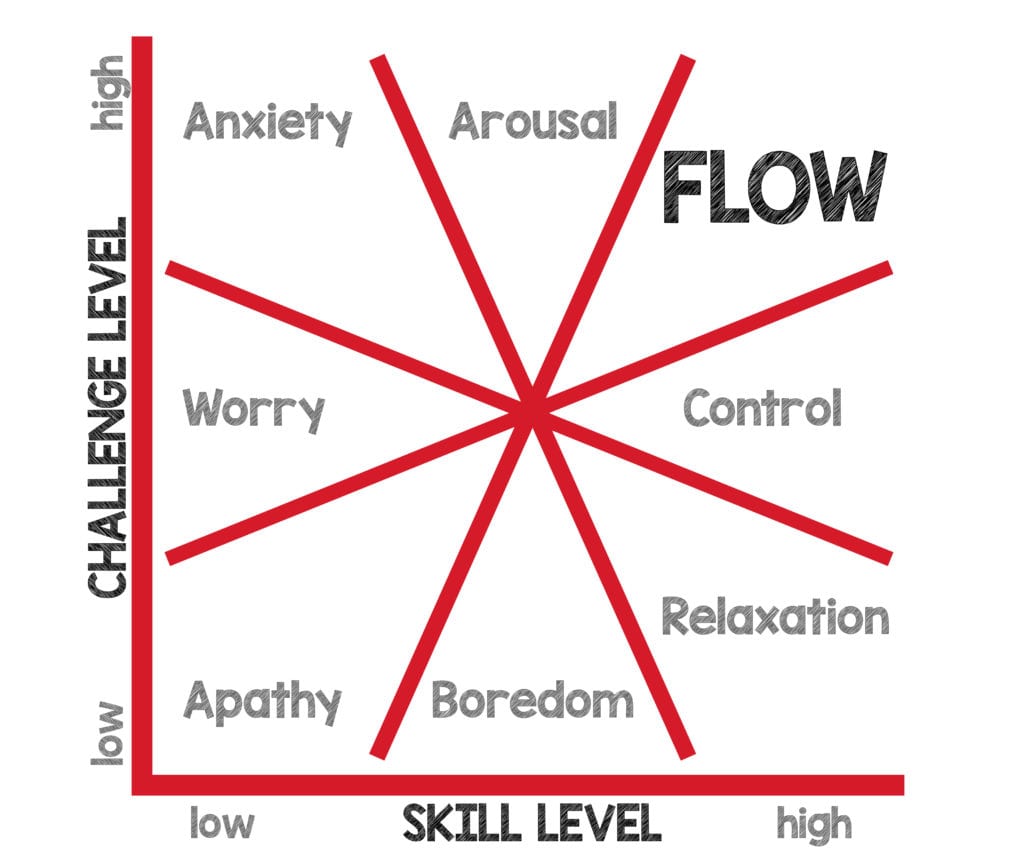
Flow exists on a spectrum between boredom and anxiety. We evoke boredom If a challenge is too easy. However, if the challenge far exceeds skill, then we trigger anxiety. We can achieve flow when challenge and skill are appropriately aligned.
COMPONENTS OF FLOW
-
- Clear Goals
- Intense concentration
- A loss of self-consciousness
- Distorted sense of time
- Direct and immediate feedback
- Ability and challenge level are aligned
- A sense of control over the situation
- The activity is intrinsically rewarding
- A lack of awareness of bodily needs
Close your eyes and picture the last patient you cared for in cardiac arrest. Did you have clear goals? Were you hyperfocused on the activity? Did you feel an awareness of self? Were you conscious of time? Was there immediate feedback? Did you have the skill? Were you in control of the situation? Did you feel thirst or hunger? Was the activity rewarding? These commonplace life-and-death ED experiences seem perfectly aligned with the components of flow.
CREATIVITY
Flow is also a creative and problem-solving state-of-being. Csikszentmihaly explains, “Every action, movement, and thought follows inevitably from the previous one.” There is tremendous creativity in medical practice, and we often refer to it as the “art of medicine.” In the ED, patients are like blank canvases free from the mark of another physician. Additionally, life-and-death situations can elicit exponential growth and creativity. The inescapable finality of death grants the freedom to attempt unproven but possibly beneficial heroic measures like double sequential defibrillation.
DANGERS OF FLOW
Flow is a universally pleasant experience, but it may not be harmless. In extreme sports, many athletes have pushed the boundaries of human capabilities and paid with their lives. In medicine, flow can also be harmful. Recall your first difficult intubation. Did you have tunnel vision or become so entrenched in placing the tube you lost track of the patient’s overall condition? In these critical situations, it’s imperative to assign roles and plan when to abort a procedure. For example, if the pulse oximeter drops below 90% stop, bag the patient, and allow a senior practitioner to make the next attempt.
HOW TO FLOW
3 conditions are needed to achieve flow:
-
- Clear goals
- Immediate feedback
- Balance between challenge and skill
Any intrinsically motivating activity can elicit flow. Have you ever become so intensely involved in a book, writing, a video game, or perhaps achieved a “runner’s high?” Then you have been in flow. Time seems to fly by when you’re in a flow state. Coincidentally, many books on productivity extol the virtues of focused work, and some specifically describe the flow state. Establishing objective goals and allocating time for deep work can facilitate flow.
The activity must be sufficiently challenging to push your capabilities and stimulate the intense focus required to enter flow. Goals and feedback are not enough. Kotler recommends a challenge 4% harder than your current abilities. While, It’s difficult to put an objective number on a creative endeavor, the aim is to push your limit.
I have ambitious year-long goals for 2021: read 50 books, write 25 blog posts, and record 12 podcasts. Again, these are ambitious, but ‘Aim high, fail high.’ I don’t have limitless bandwidth, and I face the challenges of everyday life. I have a wife, triplet toddlers, clinical and academic responsibilities, and personal hobbies. Above all, I maintain a powerful sense of what’s meaningful, and I eliminate the rest.
Monthly and weekly reviews allow me to stay focused and organized. I use a habit tracker (Productive) and an accountability mirror (Inspired by David Goggins) which allows for reflection on shortcomings. Deep Work provides the time and framework to fulfill my goals.
REFERENCES:
- Kotler, S. (2014). The rise of superman: Decoding the science of ultimate human performance. Houghton Mifflin Harcourt. [Link is here]
- Csikszentmihalyi, M., & Csikzentmihaly, M. (1990). Flow: The psychology of optimal experience (Vol. 1990). New York: Harper & Row. [Link is here]
- Csikszentmihalyi, M. (1997). Creativity: Flow and the psychology of discovery and invention. HarperPerennial, New York, 39. [Link is here]
- Deep Work: The Complete Guide (Including a Step-by-Step Checklist). Ambition & Balance. https://blog.doist.com/deep-work/. Published 2020. Accessed December 24, 2020. [Link is Here]
FOAMed Resources:
- Propersi M. Put an End Procrastination. REBEL EM Blog. Published on March 1, 2021. Available at: [Link is here]
- Propersi M. Seize the Day. REBEL EM Blog. Published on January 4, 2021. Available at: [Link is here]
- Propersi M. Shooting Azimuths. REBEL EM Blog. Published on March 15, 2021. Available at: [Link is here]
- Lauria M. Enhancing Human Performance in Resuscitation Part 1: Going With The “Flow”. EMCrit Blog. Published on December 20, 2014. Accessed on March 23rd 2021. Available at: [Link is here]
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srreziae) and Anand Swaminathan, MD (Twitter: @EMSwami)
The post The Autotelic Emergency Physician appeared first on REBEL EM - Emergency Medicine Blog.