
 Chest pain is a common presentation complaint to the emergency department (ED) and has a wide range of etiologies including urgent diagnoses (i.e. acute coronary syndrome (ACS), pulmonary embolism, aortic dissection) and non-urgent diagnoses (i.e. musculoskeletal pain, gastroesophageal reflux disease (GERD), pericarditis). The challenge in the ED is to not only to identify high risk patients but also to identify patients who can be safely discharged home. Specifically, when dealing with ACS, dynamic ECG changes or positive cardiac biomarkers is pretty much a slam dunk admission in most cases, but a lack of these does not completely rule out ACS. Currently, most guidelines and risk stratification scores focus on the identification of high risk ACS patients that would benefit from early aggressive therapies, but what about all the other chest pain patients that don’t have ACS… are they accounted for?
Chest pain is a common presentation complaint to the emergency department (ED) and has a wide range of etiologies including urgent diagnoses (i.e. acute coronary syndrome (ACS), pulmonary embolism, aortic dissection) and non-urgent diagnoses (i.e. musculoskeletal pain, gastroesophageal reflux disease (GERD), pericarditis). The challenge in the ED is to not only to identify high risk patients but also to identify patients who can be safely discharged home. Specifically, when dealing with ACS, dynamic ECG changes or positive cardiac biomarkers is pretty much a slam dunk admission in most cases, but a lack of these does not completely rule out ACS. Currently, most guidelines and risk stratification scores focus on the identification of high risk ACS patients that would benefit from early aggressive therapies, but what about all the other chest pain patients that don’t have ACS… are they accounted for?
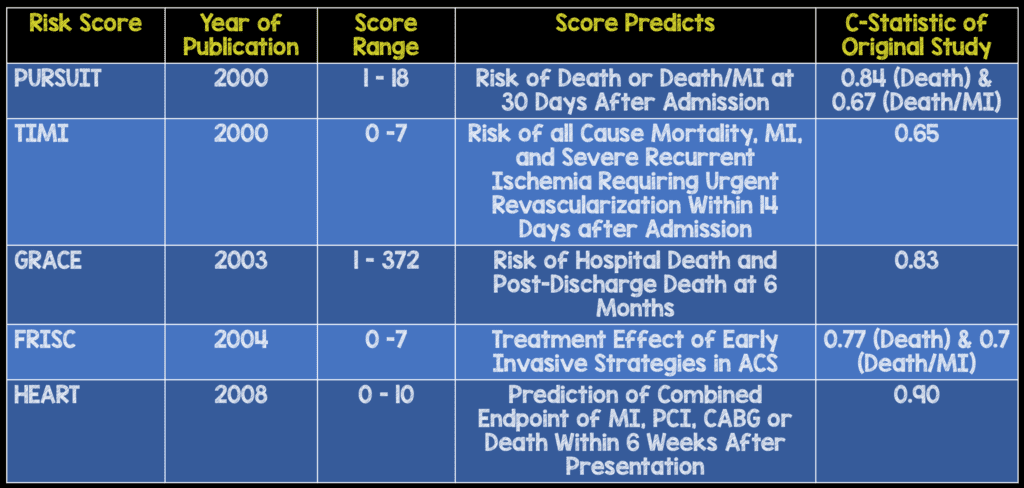
What are some of the scoring methods currently used? [1]
What is the applicability of each score to clinical practice in the ED?
- PURSUIT: Does not include troponin assays as part of score and the majority of the score is dependent on patient age.
- TIMI: Simple to use, but has a poor predictive power (i.e. c-statistic 0.65)
- GRACE: Very complex to use and a large portion of the score is dependent on the patient age. Also patients not divided into different risk groups
- FRISC: Like TIMI, is simple to use but has a poor predictive power (i.e. c-statistic 0.70)
All of the above scores are well validated, but none of them emphasizes patient history as part of the score, used in identification of ACS in the ED setting, and chest pain due to causes other than ACS were not evaluated in these trials. In truth, clinical judgement plays a huge role for physicians in the ED when evaluating chest pain patients, so wouldn’t it make sense to have a risk score that follows this? Well, that is exactly what the HEART score does!
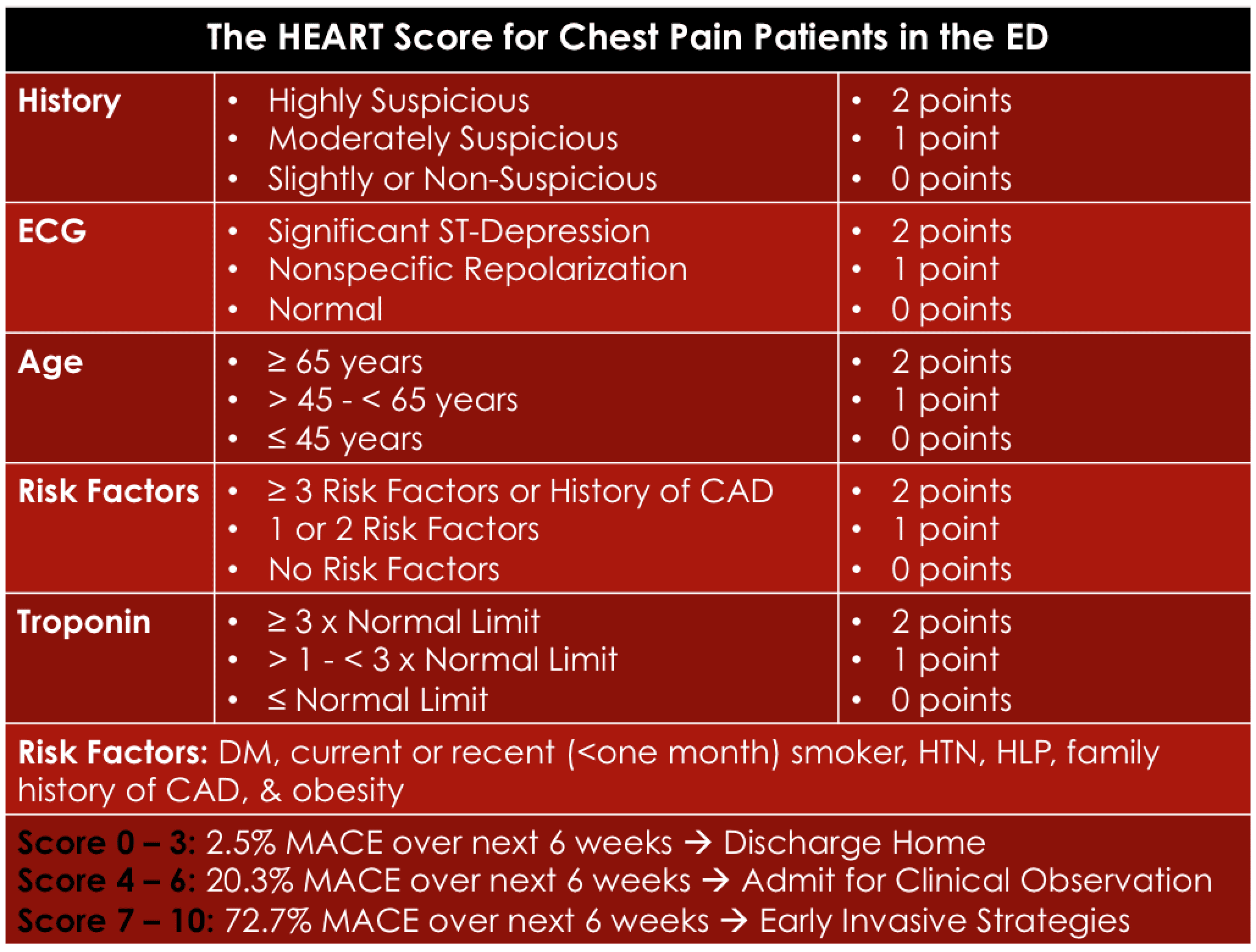
What is the HEART Score (Original Study)? [2]
Has the HEART score been validated against TIMI and GRACE scores (Validation Study)? [3]
What they did:
- 2,440 unselected, chest pain patients from 10 hospitals
- Applied TIMI, GRACE, and HEART Scores
Primary endpoint:
- Occurrence of major adverse cardiac events (MACE) at 6 weeks
- MACE = AMI, PCI, CABG, and death
Results of validation study (Different than original study shown above):
- Low HEART Score (0 -3) = 1.7% MACE Rate
- Intermediate HEART Score (4 – 6) = 16.6% MACE Rate
- High HEART Score (7 – 10) = 50.1% MACE Rate
- C-statistic of HEART Score (0.83) > TIMI (0.75) > GRACE (0.70)
Limitations:
- Study performed on patient population from the Netherlands
- Observational study
- Each ED had different cut-off values for positive troponins
- 45 patients lost to follow up
- No comparison of Heart Score to clinical gestalt
- Confidence interval was a bit wide when looking at the total study population (i.e. 2.2)
Conclusion: The HEART score provides a quick and reliable predictor of outcomes in chest pain patients presenting to the ED.
Take Home Points
- The Heart Score was developed in an ED setting in all patients with chest pain and not just ACS patients.
- A larger, prospective study with narrower confidence intervals in a US population would be nice, but best current evidence is that the HEART score performs better than TIMI and GRACE scores.
References:
- Backus BE et al. Risk Scores for Patients with Chest Pain: Evaluation in the Emergency Department. Currently Cardiol Rev 2011. PMID: 22294968
- Six AJ et al. Chest Pain in the Emergency Room: Value of the HEART Score. Neth Heart J 2008. PMID: 18665203
- Backus BE et al. A Prospective Validation of the HEART Score for Chest Pain Patients at the Emergency Department. Int J Cardio 2013. PMID: 23465250
The post The HEART Score: A New ED Chest Pain Risk Stratification Score appeared first on REBEL EM - Emergency Medicine Blog.