
 Since 2002, the surviving sepsis campaign (SSC) has stated that best practice in sepsis care includes: early recognition, source control, appropriate/timely antibiotic therapy, resuscitation with intravenous fluids (IVF) and vasoactive medications. Resuscitation of the septic patient in the emergency department has been largely based off the 2001 Rivers trial [1]. This single center study’s focus was to optimize tissue oxygen delivery following several parameters including, central venous pressure (CVP), mean arterial pressure (MAP), and central venous oxygen saturation (SCVO2) to guide IVF, vasoactive medications, and packed red blood cell (PRBC) transfusions. Well today, part 3 of the sepsis trilogy was published in the saga of Early Goal Directed Therapy (EGDT) versus “usual” care. The 3 parts to this saga consist of:
Since 2002, the surviving sepsis campaign (SSC) has stated that best practice in sepsis care includes: early recognition, source control, appropriate/timely antibiotic therapy, resuscitation with intravenous fluids (IVF) and vasoactive medications. Resuscitation of the septic patient in the emergency department has been largely based off the 2001 Rivers trial [1]. This single center study’s focus was to optimize tissue oxygen delivery following several parameters including, central venous pressure (CVP), mean arterial pressure (MAP), and central venous oxygen saturation (SCVO2) to guide IVF, vasoactive medications, and packed red blood cell (PRBC) transfusions. Well today, part 3 of the sepsis trilogy was published in the saga of Early Goal Directed Therapy (EGDT) versus “usual” care. The 3 parts to this saga consist of:
- Protocolized Care for Early Septic Shock (ProCESS) [2] – 31 Emergency Departments in the United States
- Australasian Resuscitation in Sepsis Evaluation (ARISE) [3] – 51 Emergency Departments in Australia, New Zealand, Finland, Hong Kong, and Ireland
- The Protocolised Management in Sepsis (ProMISe) Trial [4] – 56 Emergency Departments in the United Kingdom
What were the conclusions of the ProCESS and ARISE trials?
For a full description of these studies checkout: The New Age of Sepsis Management, but the synopsis of these two studies is simple and straight forward: If patients are identified EARLY, given IVF EARLY, and antibiotics EARLY, then the pathway used afterwards (i.e EGDT, Protocolized, or “usual care”) is less important in management and resuscitation.
What were the mortality rates in the EGDT study vs the ProCESS and ARISE trials?
- EGDT = 31 – 47%
- ProCESS = 18.2 – 21% 60 day mortality rate
- ARISE = 18.6 – 18.8% 90 day mortality rate
Summary: The 2001 Rivers study put sepsis on the map and has changed how we manage sepsis (i.e. We are more aggressive in identifying these patients, and our “usual care” has changed to early identification, early IVFs and early antibiotics), which may explain why we have lower mortality rates now compared to the 2001 Rivers et al study

The Protocolised Management in Sepsis (ProMISe) Trial [4]
What they did:
- Pragmatic, open, multi center, randomized controlled trial of 56 emergency departments in the United Kingdom
- 1260 patients were assigned to EGDT (6-hour resuscitation protocol) vs “usual” care
Outcomes:
- Primary: All-cause mortality at 90 days
Results:
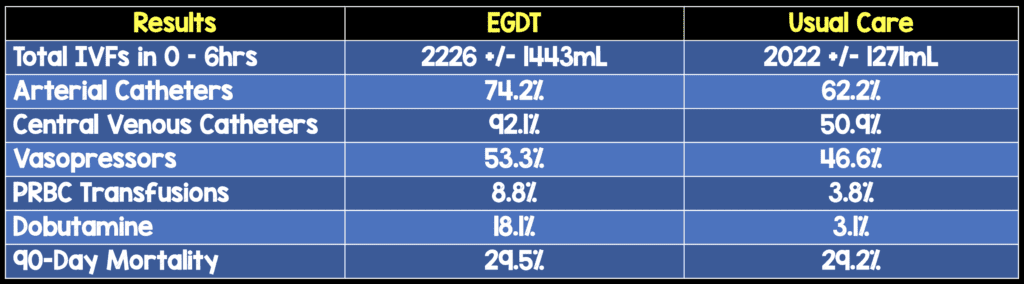
- The Sequential Organ Failure Assessment (SOFA) Score (Predictor of morbidity severity and mortality estimation) at 6 hours was higher in the EGDT arm vs “usual” care arm (6.4 +/- 3.8 vs 5.6 +/- 3.8).
- The number of patients requiring advanced cardiovascular support was 37.0% in the EGDT arm vs 30.9% in the “usual” care arm (p = 0.026)
- The number of days in the ICU was 2.6 days in the EGDT arm vs 2.2 days in the “usual” care arm (p = 0.005).
- The average cost of care was $17,647 in the EGDT arm vs $16,239 in the “usual” care arm, but this was not statistically significant (p = 0.26)
Limitations:
- Slower recruitment of patients on weekends and after business hours with only 1/3 of patients being recruited during these times
- Interventions could not be blinded, but patients were centrally randomized to conceal treatment group and ultimately minimize bias
Conclusions: In patients identified early with septic shock, the use of EGDT vs “usual” care did not result in a statistical difference in 90 day mortality.
Discussion Points from the ProMISE Study:
- This study was set in a real-world context with 29% of recruiting hospitals being teaching facilities. 20% of EDs overall in England are teaching facilities, which means the population studied, would be a generalizable sample of patients to the country as a whole
- This study calculated that an enrollment of 1260 patients would have an 80% power to detect a relative reduction of 20% in risk and absolute risk reduction of 8% in risk for the EGDT group in 90 day mortality. This study only had a 29% mortality rate as opposed to a predicted 40% mortality rate, so small differences in EGDT vs “usual” care may be missed from the results of this study
- The number of days in the ICU was 2.6 days in the EGDT arm vs 2.2 days in the “usual” care arm (p = 0.005). I am not sure of the clinical relevance of this as the difference was less than 1/2 a day.
- Looking at the results, a significant portion of “usual” care patients still get arterial catheters (62.2%), CVCs (50.9%), and vasopressors (46.6%). What this tells me is that our “usual” care has components of the EGDT algorithm engrained in it. Sick patients need fluids, antibiotics, and supportive therapies (i.e. Early critical care and resuscitation), but they don’t need CVP and SCVO2 monitoring to dictate their care .
Clinical Take Home Message:
As already confirmed by the ProCESS and ARISE trials, if patients are identified EARLY, given IVF EARLY, and antibiotics EARLY…the “ABCs” of resuscitation and critical care, then the pathway used afterwards (i.e EGDT, Protocolized, or “usual care”) the “DEF” after resuscitation is less important in the resuscitation of patients with severe sepsis and septic shock.
References:
- Rivers E et al. Early Goal-Directed Therapy in the Treatment of Severe Sepsis and Septic Shock. NEJM 2001. PMID: 11794169
- ProCESS Investigators. A Randomized Trial of Protocol-Based Care for Early Septic Shock. NEJM 2014. PMID: 24635773
- ARISE Investigators. Goal-Directed Resuscitation for Patients with Early Septic Shock. NEJM 2014. PMID: 25272316
- Mouncey PR et al. Trial of Early, goal-Directed Resuscitation for Septic Shock. NEJM 2015. PMID: 25776532
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)
Others Thoughts:
- Richard Body at St. Emlyn’s Blog: The ProMISe Study – EGDT RIP?
- Ryan Radecki at EM Lit of Note: Early Goal-Directed Waste For Sepsis
- The Bottom Line: Trial, of Early Goal-Directed Resuscitation for Septic Shock
- Thomas D at Scancrit.com: EGDT is Dead, Long Live EGDT
- Ken Milne at The Skeptics Guide to Emergency Medicine: SGEM#113 – EGDT – ProMISe(s) ProMISe(s)
The post The Protocolised Management in Sepsis (ProMISe) Trial appeared first on REBEL EM - Emergency Medicine Blog.