
 Background: Patients coming to the ED frequently have several interventions performed in their evaluation and management. Blood draws, for the most part, are venous. Occasionally, however, arterial sampling is used to gauge acid-base status, PaO2, PaCO2, lactate etc. This is a painful procedure for patients and can be challenging to perform by the staff. Although rare, ABGs can cause harm in the form of radial artery spasm, infarct, and/or aneurysms. In non-hypoxemic patients, VBGs are less painful and have been shown to have similar results compared to ABGs [2][3][4][5].
Background: Patients coming to the ED frequently have several interventions performed in their evaluation and management. Blood draws, for the most part, are venous. Occasionally, however, arterial sampling is used to gauge acid-base status, PaO2, PaCO2, lactate etc. This is a painful procedure for patients and can be challenging to perform by the staff. Although rare, ABGs can cause harm in the form of radial artery spasm, infarct, and/or aneurysms. In non-hypoxemic patients, VBGs are less painful and have been shown to have similar results compared to ABGs [2][3][4][5].
Paper: Chauvin A et al. Reducing Pain by Using Venous Blood Gas Instead of Arterial Blood Gas (VEINART): A Multicentre Randomised Controlled Trial. EMJ 2020. [Epub Ahead of Print]
Clinical Question: In non-hypoxemic patients (pulse oximetry >95% on room air), is the maximal pain during sampling less with VBG or ABG?
What They Did:
- Multicenter, open-label, randomized, prospective clinical trial in 4 French EDs over a 4-week period
- Non-hypoxemic adults, whose clinicians desired blood gas analysis to help guide care
- Randomized to arterial vs venous sampling
Outcomes:
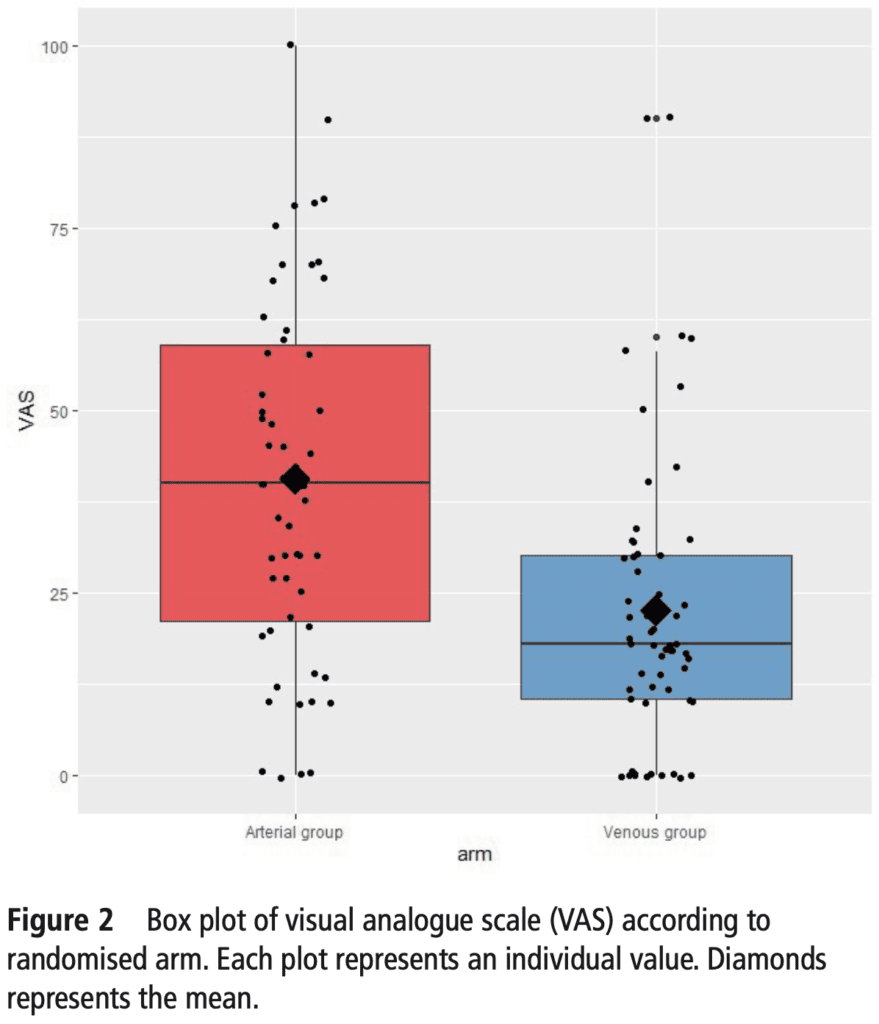
- Primary: Maximal pain during sampling using a visual analog scale (VAS) on a 0 to 100 scale
-
Secondary:
- Ease of sampling as rated by the nurse drawing the blood
- Easy
- Moderately easy
- Difficult
- Very difficult
- Physician satisfaction regarding usefulness of biochemical data
- Not at all
- Partly satisfied
- Satisfied
- Very satisfied
- Ease of sampling as rated by the nurse drawing the blood
Inclusion:
- Blood gas analysis needed based on physician decision
- Percutaneous O2 saturation >95% on room air
- Age ≥18 years
- GCS of 15
Exclusion:
- Patients under legal protection
- Unable to receive information
- No social security insurance
- Refused to participate
Results:
- 113 patients included
- Suspicion of metabolic acidosis was the main reason for blood gas analysis
- 75% of patients did not receive analgesics before the sampling (none had application of an anesthetic cream)
- None of the providers used ultrasound for sampling
-
Mean Maximal Pain (Primary Outcome):
- ABG: 40.5mm +/- 24.9mm
- VBG: 22.6mm +/- 20.2mm
- Absolute Difference: 17.9mm (95% CI 9.6 to 26.3; p<0.0001)
- Ease of blood sampling greater with VBG vs ABG (p = 0.02)
- 1st attempt success: VBG 91% vs ABG 80%
- Blood sampling assessed as easy: VBG 69% vs ABG 44%
- Blood sampling assessed as difficult: VBG 3% vs ABG 15%
- Usefulness of results did not differ (p = 0.25)
- Physician satisfaction with usefulness of information satisfying or very satisfying: VBG 95% vs ABG 97%
Strengths:
- Asks a clinically important question
- 1st randomized clinical trial assessing pain experienced by patients for ABG vs VBG in the ED setting
- Multicenter, randomized clinical trial
- Patients were asked their VAS pain score within 3 minutes of the blood draw to reduce recall bias
- Almost all patients received their allocated intervention (1 patient did not in the ABG group)
- No patients were lost to follow up
- Performed two post-hoc sensitivity analyses to account for the corresponding group in which actual blood sampling technique was used and for baseline imbalance despite randomization
Limitations:
- Patients were imbalanced at baseline in regard to age, medical history, and diagnosis hypotheses motivating blood sampling.
- Diameter of the arterial puncture needle was 22G for ABG and varied for VBGs between 20 and 25G. Smaller gauge needles will cause less pain than larger gauge needles
- Outcome assessments were not blinded which could bias the results of the physician (This should not bias the results of the patients)
- 64 patients were not consented out of 177 eligible patients. This is more of a convenience sample than a consecutive sample.
- Years of professional experience and comfort with the procedures was not recorded in this study
- Patients were not treated equally. 25% had analgesia prior to sampling but this wasn’t standard practice
- VAS pain scales are a subjective scale of pain and may differ between patients
Discussion:
- A clinically relevant difference was set at a VAS of at least 20mm and a SD of the difference of 28mm. However the authors only found an 18% difference between groups. As the study was not truly powered to detect this small a difference, this could be statistical noise and a much larger study would be needed to delineate this
- Peripheral venous lactate determination cannot be substituted for arterial lactate determination in all cases. Agreement between VBG and ABG values can decline when venous lactate is ≥2mmol/L. This can result in a greater difference in agreement between samples. A normal lactate level on venous lactate does however rule out increased arterial lactate concentrations
Author Conclusion: “Venous blood gas is less painful for patients than ABG in non-hypoxaemic patients. Venous blood gas should replace ABG in this setting.”
Clinical Take Home Point: In non-hypoxemic patients requiring acid-base evaluation:
- VBG is less painful for patients compared to ABG
- VBG is easier for the healthcare team compared to ABG
- VBG provides useful information similar to ABG for physicians in regard to treatment decisions
References:
- Chauvin A et al. Reducing Pain by Using Venous Blood Gas Instead of Arterial Blood Gas (VEINART): A Multicentre Randomised Controlled Trial. EMJ 2020. [Epub Ahead of Print]
- Kelly AM et al. Review Article – Can Venous Blood Gas Analysis Replace Arterial in Emergency Medical Care. Emerg Med Australas 2010. PMID: 21143397
- Razi E et al. Correlation of Arterial Blood Gas Measurements with Venous Blood Gas Values in Mechanically Ventilated Patients. Tanaffos 2012. PMID: 25191435
- McCanny P et al. Venous vs Arterial Blood Gases in the Assessment of Patients Presenting with an Exacerbation of Chronic Obstructive Pulmonary Disease. AJEM 2012. PMID: 21908141
- Zeserson E et al. Correlation of Venous Blood Gas and Pulse Oximetry with Arterial Blood Gas in the Undifferentiated Critically Ill Patient. J Intensive Care Med 2018. PMID: 27283009
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)


The post The VEINART Trial: VBG vs ABG appeared first on REBEL EM - Emergency Medicine Blog.