
 Background: Patients who present with a transient ischemic attack (TIA) are at higher risk of subsequent stroke, especially in the short term (< 7 days). However, the majority of these patients do not experience strokes which leads to a clinical conundrum; should all TIAs be admitted for evaluation? Comprehensive investigation, aggressive treatment, and/or hospital admission is not feasible for all patients and being able to risk stratify these patients to those who would most likely benefit is crucial.
Background: Patients who present with a transient ischemic attack (TIA) are at higher risk of subsequent stroke, especially in the short term (< 7 days). However, the majority of these patients do not experience strokes which leads to a clinical conundrum; should all TIAs be admitted for evaluation? Comprehensive investigation, aggressive treatment, and/or hospital admission is not feasible for all patients and being able to risk stratify these patients to those who would most likely benefit is crucial.
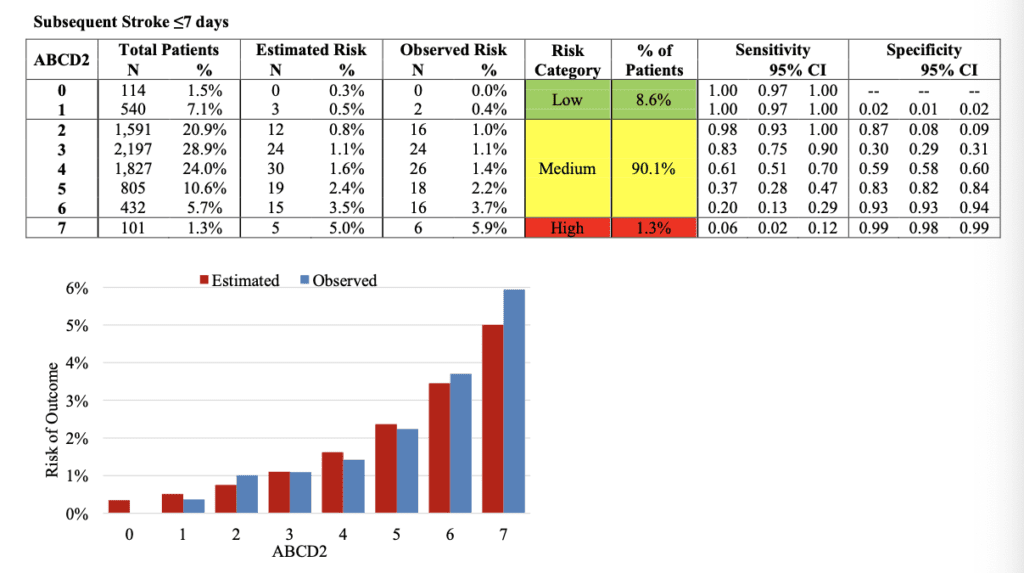
The ABCD2 score, one of the best-known scores for TIA decision making, has performed sub-optimally in validation studies. The score has shown low sensitivity for identifying low risk patients, and low specificity for identifying high risk patients [3]. Clearly, better decision instruments are needed.
Paper: Perry JJ et al. Prospective Validation of Canadian TIA Score and Comparison with ABCD2 and ABCD2i for Subsequent Stroke Risk After Transient Ischaemic Attack: Multicentre Prospective Cohort Study. BMJ 2021. [Link is HERE][Access on Read by QxMD]
Clinical Question: Does the Canadian TIA Score perform better than the ABCD2 score in stratifying subsequent stroke risk in patients with TIAs?
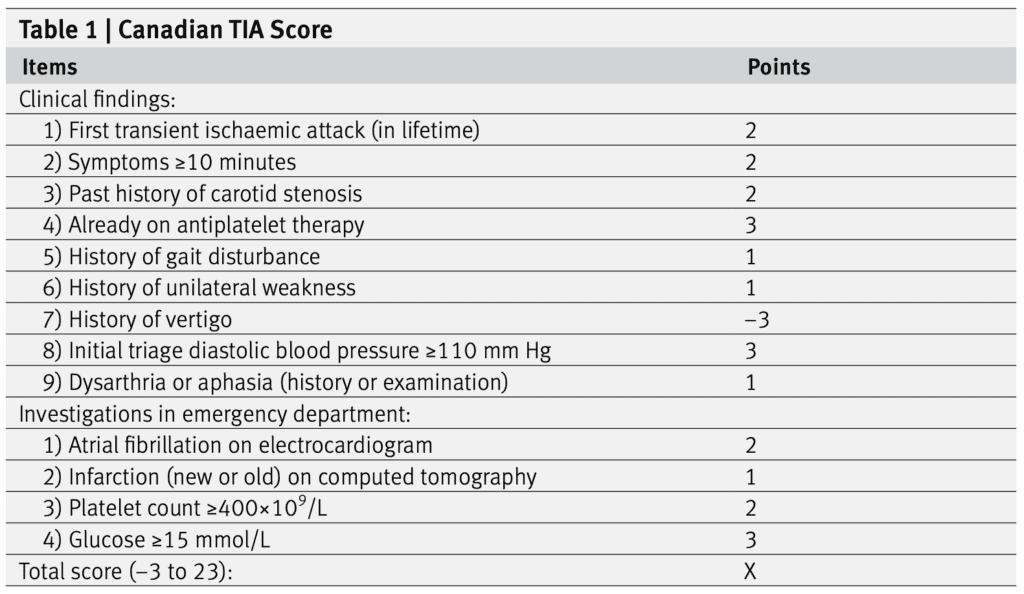
Canadian TIA Score
- Score range: -3 to 23
- Gives a graded probability of stroke over the next 7d of 0.01% up to 28%
- Low risk: -3 to 3
- Medium Risk: 4 to 8
- High Risk: ≥9
What They Did:
- Prospective multicenter cohort study
- 13 Canadian EDs over 5 years
- Validation of previous derivation study of the Canadian TIA score [2]
- Followed patients up for 7d and 90d after index visit
- 3 things were then done:
- Calculated sensitivity and specificity at each integer value from -3 to 23 of the Canadian TIA score
- Assessed risk in low, medium and high-risk groups in the Canadian TIA score, ABCD2 score, and ABCD2i score
- Compared performance of Canadian TIA score against ABCD2 and ABCD2i
Outcomes:
- Primary: Subsequent stroke or carotid endarterectomy/carotid artery stenting within 7d
-
Secondary:
- Subsequent stroke within 7d (with or without carotid endarterectomy/carotid artery stenting)
- Telephone follow up for verifying stroke free status at 7 and 90d
Inclusion:
- ≥18 years of age
- TIA or minor stroke as final ED diagnosis
Exclusion:
- Neurological deficits >24hrs
- Decreased GCS from baseline
- Alternative diagnosis (i.e. hypoglycemia, seizure, etc…)
- Presentation >7d after onset of neurological symptoms
- Treated with tPA or embolectomy for acute stroke
Results:
- 7607 consecutively enrolled adult patients (80.6% of all potentially eligible patients)
- 108 (1.4%) had a subsequent stroke within 7d
- 83 (1.1%) had carotid endarterectomy/carotid artery stenting within 7d
- 9 patients had both within 7d leaving 182 with outcomes
- Only 5.8% of patients admitted to the hospital from the ED at the time of index visit
- Number of patients that fell into each risk group:
- Low risk: 16.3% of patients
- Medium Risk: 72.1% of patients
- High Risk: 11.6% of patients
-
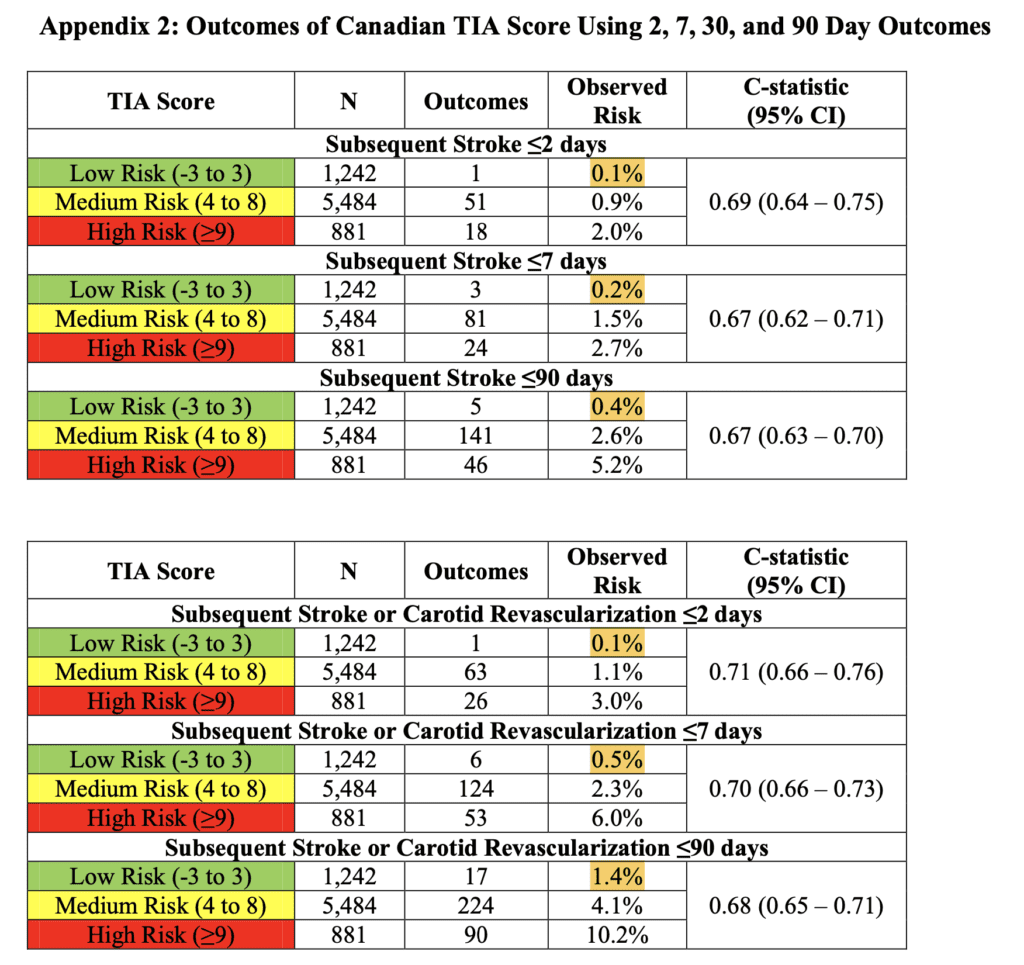
Canadian TIA Score
- Authors use something called interval likelihood ratios (I had to look this term up):
- This is simply making diagnostic decisions based on a test result represented on a continuous scale
- When results of continuous data are expressed as binary outcomes using a single cutoff, distortion of data can occur because markedly abnormal values are lumped together with results that are only mildly abnormal
- Interval likelihood ratios provide a better analysis than sensitivity and specificity because they assign a specific value to each level of abnormality which can be used to calculate posttest probability of disease for a given level of a test
-
Stratified Risk of Stroke, Carotid Endarterectomy/Carotid Artery Stenting or Both Within 7d (Primary Outcome):
- Low risk: ≤0.5%; Interval LR 0.2; 95% CI 0.09 to 0.44
- Medium risk: 2.3%; Interval LR 0.94; 95% CI 0.85 to 1.04
- High risk: 5.9%; Interval LR 2.56; 2.02 to 3.25
- Authors use something called interval likelihood ratios (I had to look this term up):
- Neither the ABCD2 nor the ABCD2i score was able to classify any patients as being low risk for the primary outcome (<1% for subsequent stroke or carotid revascularization within 7d)
- ABCD2 and ABCD2i and Stroke ≤7d
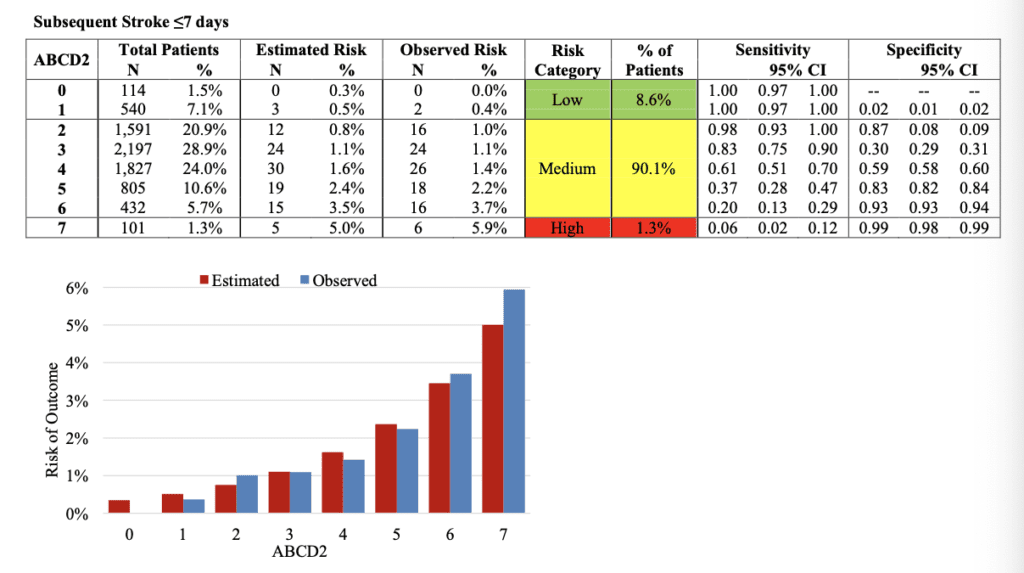
- Canadian TIA Score was more accurate than the ABCD2 and ABCD2i scores
- Canadian TIA Score: AUC 0.70; 95% CI 0.66 to 0.73
- ABCD2 Score: AUC 0.60; 95% CI 0.55 to 0.64
- ABCD2i Score: AUC 0.64; 95% CI 0.59 to 0.68
Strengths:
- Asks a clinically important question
- Consecutive patients enrolled over 5 years
- Minimal exclusions make results more generalizable
- Needed 5000 patients collected 7600 patients
- Included both community and academic centers
- Included six new sites that were not involved in the derivation study
- All outcomes were adjudicated by panels of 3 stroke experts, who were blinded to the index ED visit
- Used pre-specified risk thresholds (low risk <1%, medium risk 1 to 5%, and high risk >5%) based on previous surveys of ED physicians and neurologists
- Near complete follow up with only 34 (0.4%) of patients missed by 7d
- Largest enough sample size to look at precision of subsequent stroke alone without considering carotid revascularization
Limitations:
- Canadian TIA score is a more complicated score to calculate compared to ABCD2
- 20% of eligible patients were not enrolled (unclear why this occurred)
- Overall rate of outcome was low which would overestimate the performance of a clinical decision instrument since it was such a low-risk group
- Used a composite outcome of a procedure (carotid revascularization) which is a subjective decision and subsequent stroke which is an objective diagnosis as the primary outcome
- Validation study done by the same group, in the same Canadian health system. Would like to see this risk stratification applied to systems with different healthcare systems
- Canadian TIA risk score was not compared to clinician gestalt
Discussion:
- Validation of a clinical decision rule improves believability in applying this instrument to other cohorts of patients
- ABCD2 and ABCD2i classified all but 3 to 7% of patients into a medium risk for the primary outcome, which is clinically not helpful. These scores were designed to be dichotomous scores (low risk vs high risk), therefore patients in the medium risk category would need admission and advanced imaging.
- Carotid revascularization in patients with high grades of carotid disease has increased in management of TIAs over the past decade. This was not incorporated into the original ABCD2 score
- ABCD2i was better than ABCD2 at identifying patients at low risk for subsequent stroke, but missed many patients who would have undergone early carotid revascularization
- One of the big keys to risk stratification working is the system in which one works. If neurology follow up and MRI/MRA imaging of the head and neck can be done in 24 to 48 hours, this is a great way to decrease hospitalizations. However, in the US this is not the case and regardless of what risk category a patient falls in, medicolegal pressures, would advocate for admission for expedited workup as in many institutions next day follow up is not possible or even feasible
- Additionally, lower/higher risk stratification is one thing but does not mean admission/obs is the right thing to do because it is unclear if we can change the outcome by hospitalization. Simply starting aspirin or dual anti-platelet therapy may be modification enough until further outpatient workup can be performed
- At the very end of the paper, the authors give clinical implications of using the Canadian TIA risk score:
- Low Risk: Non-contrast head CT with outpatient follow up
- Medium Risk: Non-contrast head CT + CTA of head/neck + rapid follow up
- High Risk: Non-contrast head CT + CTA of head/neck + neurology consultation in the ED
Author Conclusion: “The Canadian TIA Score stratifies patients’ seven day risk for stroke, with or without carotid endarterectomy/carotid artery stenting, and is now ready for clinical use. Incorporating this validated risk estimate into management plans should improve early decision making at the index emergency visit regarding benefits of hospital admission, timing of investigations, and prioritization of specialist referral.”
Clinical Take Home Point: As they always do, Perry and colleagues have done an amazing job deriving and validating the Canadian TIA Score. This score is certainly better than ABCD2 and ABCD2i in risk stratification of patients with suspected TIAs. However, risk stratification is one thing, and the resources available, follow up available, and the health system in which one works may make risk stratification a moot point.
References:
- Perry JJ et al. Prospective Validation of Canadian TIA Score and Comparison with ABCD2 and ABCD2i for Subsequent Stroke Risk After Transient Ischaemic Attack: Multicentre Prospective Cohort Study. BMJ 2021. [Link is HERE][Access on Read by QxMD]
- Perry JJ et al. A Prospective Cohort Study of Patients with Transient Ischemic Attack to Identify High-Risk Clinical Characteristics. Stroke 2014. PMID: 24262323
- Perry JJ et al. Prospective Validation of the ABCD2 Score for Patients in the Emergency Department with Transient Ischemic Attack. CMAJ 2011. PMID: 21646462
For More Thoughts on This Topic Checkout:
- St. Emlyn’s Blog: Canadian TIA Risk Score
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami)


The post TIA Risk Stratification: The Canadian TIA Score vs ABCD2 appeared first on REBEL EM - Emergency Medicine Blog.