
 Goals of lung protective mechanical ventilation: Minimizing harm during mechanical ventilation with a lung-protective strategy with:
Goals of lung protective mechanical ventilation: Minimizing harm during mechanical ventilation with a lung-protective strategy with:
- Low tidal volume (TV)
- Limit plateau pressure to <30mmHg
- Optimal positive end expiratory pressure (PEEP) set to decrease driving pressure
REBEL Crit Cast Episode 4.0 – Lung Protective Mechanical Ventilation
Low Tidal Volume
- Typical acute respiratory distress syndrome (ARDS): Ventilating small proportion of lung volume (functional lung size – “baby lungs”)
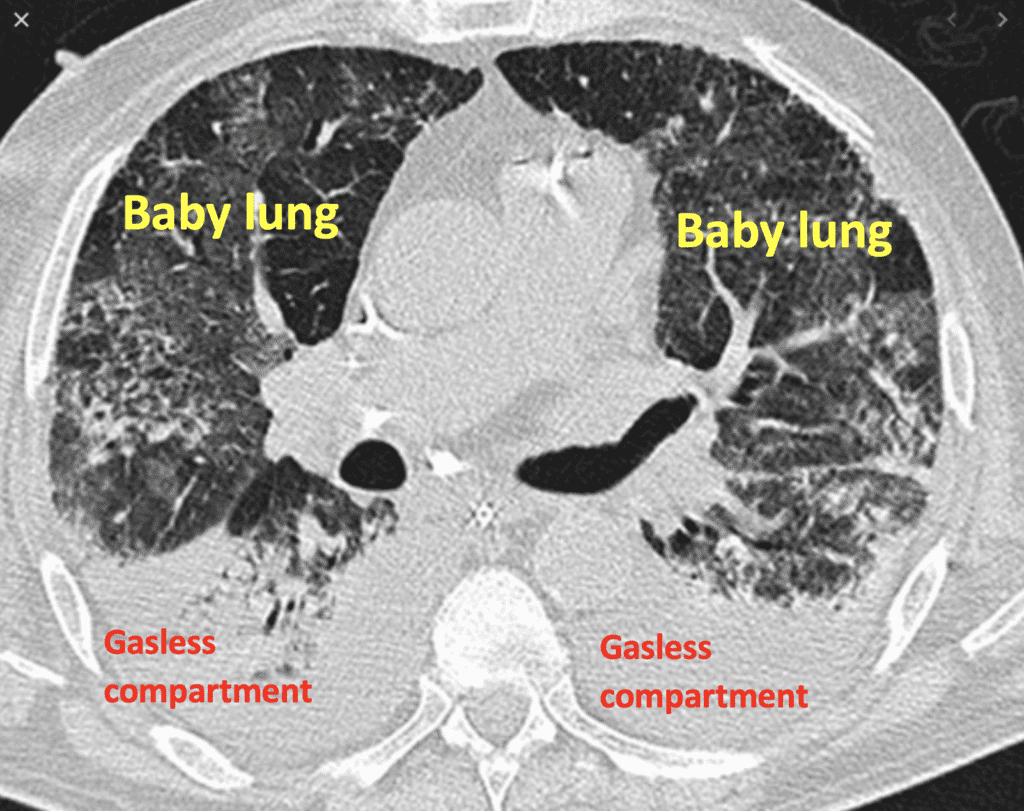
- Don’t want to over-inflate good lung and cause injury
- 8cc/kg of Ideal Body Weight (IBW; set for gender and height) may be protective in a person with normal lungs
- However, if a patient has a process with increased risk for development of ARDS, the goal is to minimize TV with the assumption they may progress to ARDS
- Target TV 6cc/kg or less of IBW
Limiting Plateau Pressure
- Plateau pressure (PPlat) = Alveolar distending pressure (static pressure which reflects lung compliance)
- e., the pressure seen by the small airways or alveoli
- Too high of PPlat may lead to barotrauma
- Goal PPlat < 30mmHg
- Way to obtain PPlat: inspiratory pause (ventilator maneuver)
- An important pressure as it reflects the pressure in the alveoli
Optimal PEEP
- PEEP is protective, and setting it optimally is important so that during expiration, alveoli do not collapse (atelectasis) which will help maintain adequate alveolar surface area for oxygen diffusion to continue
- However, no study has shown that high PEEP is protective
- Optimal PEEP can minimize driving pressures
Amato and colleagues “Driving Pressure and Survival in the Acute Respiratory Distress Syndrome” [1]

Driving pressure (∆P) = Vt/CRS (Tidal Volume/Compliance)
- Think of this as optimizing mechanical ventilation in ARDS that adapts to the size of the aerated portion of the lungs
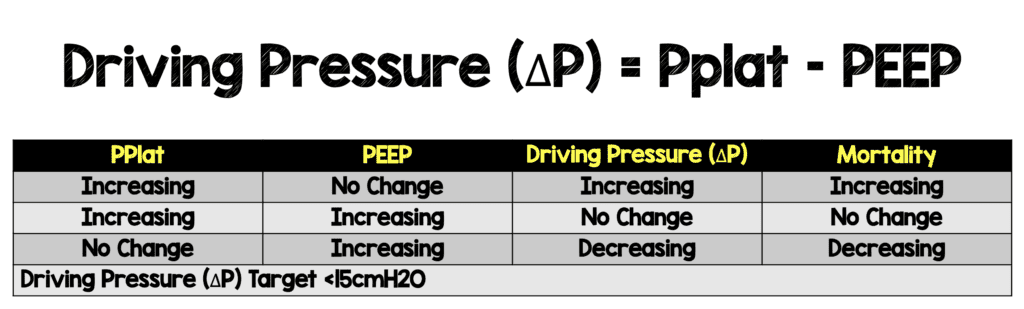
- Driving pressure (∆P) = PPlat – PEEP
- Goal driving pressure < 15mmHg BUT the lower the better!
- Compliance can be thought of as the “stiffness” of the lung
- Consider a stiff lung (low compliance) with a set TV
- If compliance decreases, you are going to need higher driving pressure (∆P), which is associated with higher mortality
- Constant PEEP with increased ∆P associated with higher mortality (Panel A above)
- Constant ∆P with increased PEEP & PPlat associated no difference in mortality (Panel B above), so higher PPlat didn’t matter if ∆P stayed constant
- Constant PPlat but increased ∆P was associated with increased mortality (Panel C above)
- Driving pressure was associated with mortality more so than any other variable
Harm of too low a PEEP
- Imagine a patient: newly intubated, with a set respiratory rate (RR) of 20. This is 20 breaths/min x 60min x 24hr = 28,800 breaths/day you allowed the alveoli to collapse and re-open!
- This causes shear stress on alveoli, or atelectotrauma
- Need optimal PEEP to limit pressure seen on alveoli

- Simply increasing PEEP based on FiO2% to improve oxygenation outside of ARDS physiology as described in some cases of COVID-19 may be harmful
- Thus, it may be more helpful to look at driving pressure, as opposed to O2 saturation, or P/F ratio as per typical ARDS protocols
- Setting optimal PEEP may minimize driving pressure, even if plateau pressure increases
Driving pressure (∆P) can be measured by [Plateau pressure – PEEP]
- Example: newly intubated patient
- Set Volume-Control mode with 6cc/kg IBW
- How to calculate optimal PEEP:
- Set PEEP to 8 and measure plateau pressure to be 25
- Driving pressure = (plateau pressure – PEEP) = (25 – 8) = 17
- Increase PEEP to 10, and subsequently measure plateau pressure of 26
- New driving pressure = 26 – 10 = 16
-
Increase PEEP to 12, plateau pressure 26
- New driving pressure = 26 – 12 = 14 (OPTIMAL PEEP)
- Increase PEEP to 14, plateau pressure 31
- New driving pressure = 31 – 14 = 17
- Set PEEP to 8 and measure plateau pressure to be 25
Clinical Bottom Line:
In summary, lung protective strategies for mechanical ventilation include limiting TV, plateau pressure to <30 mm Hg, and optimizing PEEP to reduce driving pressures (∆P). Driving pressure can be calculated at the bedside using the formula (plateau pressure – PEEP), with a goal of <15 but the lower the better. You can try this daily, or twice daily to obtain optimal PEEP to minimize driving pressures and prevent lung injury.
Guest Post With

Jeffery Rickert DO
References:
- Amato MB et al. Driving Pressure and Survival in the Acute Respiratory Distress Syndrome. NEJM 2015. PMID: 25693014
- Frank Lodeserto MD, “Simplifying Mechanical Ventilation – Part 1: Types of Breaths”, REBEL EM blog, March 8, 2018. [Link is HERE]
- Frank Lodeserto MD, “Simplifying Mechanical Ventilation – Part 2: Goals of Mechanical Ventilation & Factors Controlling Oxygenation and Ventilation”, REBEL EM blog, May 18, 2018. [Link is HERE]
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post REBEL Crit Cast Ep 4.0: Lung Protective Mechanical Ventilation appeared first on REBEL EM - Emergency Medicine Blog.