
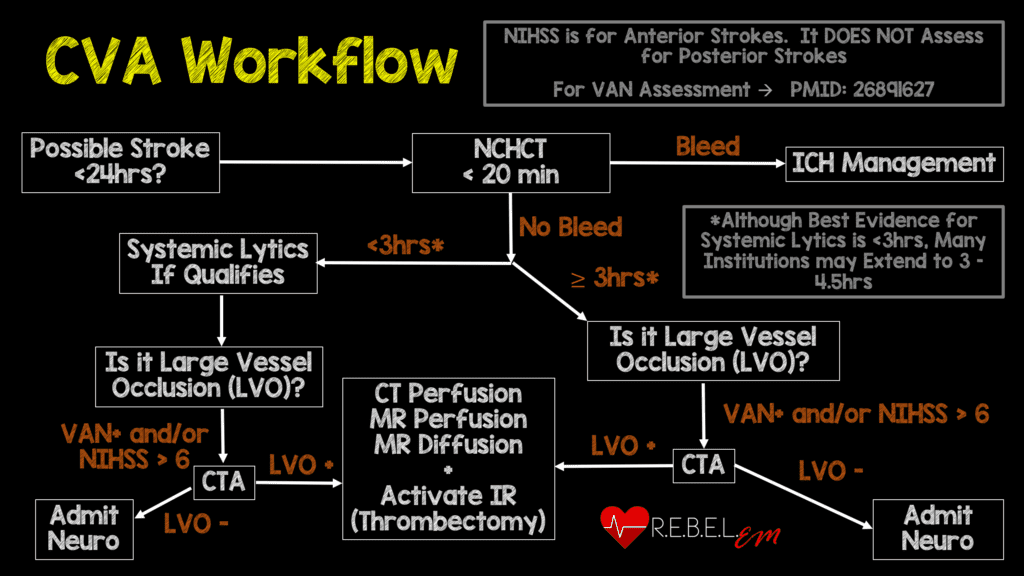
 Background: The publication of the MR CLEAN trial in January 2015 changed the face of ischemic stroke care. This was the first study demonstrating a benefit to endovascular treatment of a specific subset of ischemic stroke patients: those with a large vessel occlusion (LVO) presenting within 6 hours of symptom onset. MR CLEAN was followed by a flurry of publications seeking to replicate and refine treatment as well as expand the window for treatment. The REBEL EM team reviewed this literature back in 2018 and, with the help of Dr. Evie Marcolini, created a workflow (shown below).
Background: The publication of the MR CLEAN trial in January 2015 changed the face of ischemic stroke care. This was the first study demonstrating a benefit to endovascular treatment of a specific subset of ischemic stroke patients: those with a large vessel occlusion (LVO) presenting within 6 hours of symptom onset. MR CLEAN was followed by a flurry of publications seeking to replicate and refine treatment as well as expand the window for treatment. The REBEL EM team reviewed this literature back in 2018 and, with the help of Dr. Evie Marcolini, created a workflow (shown below).
One major component of LVO management is the use of systemic thrombolytics in patients presenting within the current thrombolytic treatment window prior to endovascular intervention. However, it’s unclear if systemic thrombolytic administration results in better outcomes or if it simply exposes the patient to increased risks at a higher cost. Limited evidence questions the utility of the current approach with lytics + endovascular therapy (Phan 2017, Rai 2018). There is a clear need for further research into systemic thrombolytics dosing and use.
Article: Yang P et al. Endocascular thrombectomy with or without intravenous alteplase in acute stroke. NJEM 2020. PMID: 32374959
Clinical Question: Is endovascular therapy alone non-inferior to endovascular therapy + systemic thrombolytics in the treatment of patients with large vessel occlusion (LVO) strokes presenting within 4.5 hours of onset?
Population: Adult patients presenting within 4.5 hours of ischemic stroke symptom onset and with cerebral vascular occlusion on CT angiography of the intracranial internal carotid artery or middle cerebral artery (first and/or second segments) and an NIHSS > 2 and if endovascular thrombectomy was intended to be performed.
Outcomes:
- Primary: modified Rankin scale (mRS) assessed at 90 days after randomization looking for non-inferiority (defined as a lower end of the odds ratio > 0.80)
-
Secondary:
- Death from any cause at 90 days
- Successful reperfusion before thrombectomy
- Recanalization at 24-72 hours (assessed by CTA)
- NIHSS score at 24 hours, and 5-7 days
- Final lesion volume on CT
- mRS comparisons
-
Safety Outcomes
- All hemorrhages and symptomatic intracranial hemorrhages according to the Heidelberg criteria
- Occurrence of pseudoaneurysm and groin hematoma at the site of arterial puncture used for thrombectomy
- Cerebral infarction in a new vascular territory at 5 to 7 days
- Mortality within 90 days
Intervention: Endovascular thrombectomy alone
Control: Endovascular thrombectomy + systemic alteplase 0.9 mg/kg
Design: Multicenter, randomized, non-blinded prospective study.
Excluded:
- Prior disability before the stroke (mRS > 2)
- Contraindication to intravenous alteplase
Primary Results:
-
- 1586 patients screened across 41 academic centers in China over 16 months
-
656 patients enrolled
- 327 to thrombectomy-alone + 329 to combination treatment
- 639 patients underwent groin puncture
- 591 patients underwent endovascular thrombectomy
-
Major protocol violations
- N = 25
- No groin puncture: n = 17
- Crossover: n = 4 in each group
- 319/329 patients in the combination group received alteplase
- Median age = 69 years
- Median NIHSS score = 17
- Median time from onset to randomization: 167 minutes (thrombectomy alone) vs 177 minutes (combination)
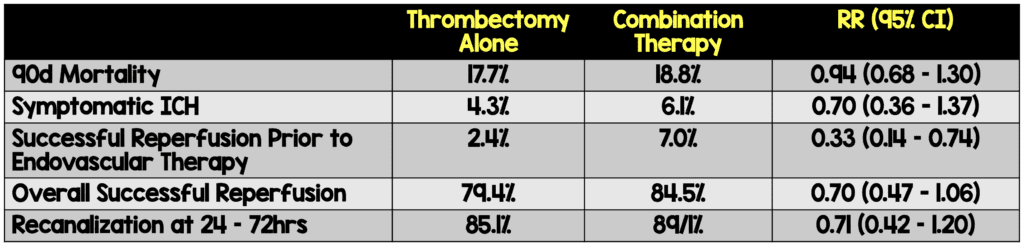
Critical Findings:
-
-
Primary outcome (adjusted odds ratio for the mRS)
- aOR = 1.07 (95% CI 0.81 TO 1.40)
- Demonstrates non-inferiority as lower limit of non-inferiority was set at 0.80
- Secondary outcomes
-
Primary outcome (adjusted odds ratio for the mRS)
Strengths:
- Study asks an important clinical question that has implications for patient outcomes as well as resource utilization
- The study was performed across multiple institutions which increases external validity
- Primary outcome is patient centered (function) as opposed to disease oriented (ie reperfusion)
- Randomization was adequately performed, and baseline characteristics are well balanced
- All sites were experienced with end-vascular therapy – required to perform at least 30 procedures in last year
- Although patients and clinicians were not blinded to the use of alteplase, both outcome assessors and radiologists reviewing scans for reperfusion and infarct size were blinded to treatment arm
Limitations:
- Though the mRs is a well-accepted outcome measure, there is some subjectivity to it which threatens the validity of the data
- The study was only performed in academic centers and only in China which decreases external validity
- A substantial number of eligible patients declined to participate (n = 240) and demographic data on this group is unavailable
- It is unclear if patients were recruited consecutively or not
- Outcome data were obtained via interviews performed in person or by phone. Phone interviews are suboptimal for assessing functionality
Discussion:
- Prior to this well-done, relatively large randomized trial, we only had retrospective, non-randomized data (Phan 2017, Rai 2018) looking at this question. The evidence from Yang et al appears to echo the prior lower quality data
- The prespecified non-inferiority margin was relatively large (20% difference in OR). A larger study with a smaller margin may still reveal a benefit to combination treatment.
- The proportion of patients with early reperfusion in this trial was similar to that reported in the control group of the Tenecteplase versus Alteplase be- fore Endovascular Therapy for Ischemic Stroke (EXTEND-IA TNK) trial, but it was lower than that reported in the tenecteplase group of that trial. Perhaps tenecteplase is a better thrombolytic option.
- In the absence of a clear benefit to systemic thrombolytics, their use must be questioned as they increase risk to the patient (intracranial and extracranial hemorrhage, early death) and increase costs (US cost ~ 6.5K)
- Application of this data to locations where endovasular therapy is only available after transfer to a larger center must be made cautiously. In a comprehensive stroke center, time from door to groin puncture will be shorter than what would be seen if transfer required. Whether this makes a difference regarding use of systemic lytics is unknown.
- The authors note that older technology was utilized in this study and that the use of more recent endovascular devices may affect results
- Alteplase infusion was ongoing during the endovascular procedure in 86.5% of the patients. This may explain why pre-endovascular reperfusion was so low.
Authors Conclusions:
“In Chinese patients with acute ischemic stroke from large-vessel occlusion, endovascular thrombectomy alone was noninferior with regard to functional outcome, within a 20% margin of confidence, to endovascular thrombectomy preceded by intravenous alteplase administered within 4.5 hours after symptom onset.”
Our Conclusions: In this relatively large, well-done trial, thrombectomy alone was non-inferior to thrombectomy + systemic thrombolytics in the treatment of LVO strokes.
Potential to Impact Current Practice: Additional studies are needed but, given the potential harms of systemic thrombolytics, they should not be used in patients who can immediately be taken for endovascular intervention. Further research is needed regarding patients who are in a “drip and ship” model.
For More on This Topic Checkout:
- REBEL EM: Endovascular Therapy for Acute Ischemic Stroke
- EM Lit of Note: Settling the Thrombolysis Before Thrombectomy Question
- The SGEM: With or Without You – Endovascular Treatment With or Without tPA for Large Vessel Occlusions
- The Bottom Line: DIRECT-MT
References:
- Phan K et al. Endovascular thrombectomy alone versus combined with intravenous thrombolysis. World Neurosurg 2017; 108: 850-8. PMID: 28823660
- Rai AT et al. Intravenous thrombolysis before endovascular therapy for large vessel strokes can lead to significantly higher hospital costs with our improving outcomes. J Neurointerv Sure 2018; 10(1): 17-21. PMID: 28062805
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post The DIRECT-MT Trial: Are Systemic Lytics Necessary in LVO Treatment? appeared first on REBEL EM - Emergency Medicine Blog.