
Background Information:
 Atrial fibrillation with rapid ventricular rate (RVR) is one of the many tachydysrhythmias we encounter in the Emergency Department (ED). Though consensus has been reached for first-line treatment of ventricular rate control1 with beta blockers (BB) and non-dihydropyridine (non-DHP) calcium channel blockers (CCB), there is still much debate regarding a preferred second-line agent for ventricular rate control. Based on 2019 American Heart Association (AHA) guidelines, amiodarone and digoxin have been suggested as alternative options in controlling ventricular rate refractory to first-line BBs and non-DHP CCBs.2 Amiodarone is commonly known for its anti-arrhythmic properties and a commonly used agent in the Intensive Care Unit (ICU). However, digoxin is known for its rate-control properties and its direct vagal effect on the atrioventricular node.3 The authors of this study sought to compare intravenous (IV) amiodarone to IV digoxin as a second-line agent in ED patients with atrial fibrillation or flutter refractory to BBs or non-DHP CCBs.
Atrial fibrillation with rapid ventricular rate (RVR) is one of the many tachydysrhythmias we encounter in the Emergency Department (ED). Though consensus has been reached for first-line treatment of ventricular rate control1 with beta blockers (BB) and non-dihydropyridine (non-DHP) calcium channel blockers (CCB), there is still much debate regarding a preferred second-line agent for ventricular rate control. Based on 2019 American Heart Association (AHA) guidelines, amiodarone and digoxin have been suggested as alternative options in controlling ventricular rate refractory to first-line BBs and non-DHP CCBs.2 Amiodarone is commonly known for its anti-arrhythmic properties and a commonly used agent in the Intensive Care Unit (ICU). However, digoxin is known for its rate-control properties and its direct vagal effect on the atrioventricular node.3 The authors of this study sought to compare intravenous (IV) amiodarone to IV digoxin as a second-line agent in ED patients with atrial fibrillation or flutter refractory to BBs or non-DHP CCBs.
Paper: Mason JM, et al. Amiodarone versus digoxin for acute rate control of atrial fibrillation in the emergency department. Am J Emerg Med. 2022. PMID: 36115743
Clinical Question:
What is the effectiveness of IV amiodarone vs IV digoxin used as second line therapy in critically ill emergency department patients with atrial fibrillation/flutter where first-line BB use has failed?
What They Did:
- Single-center retrospective study performed at an academic tertiary care center between April 2016 and March 2022 in Boston, MA
- Included patients were assigned to one of two groups
- IV amiodarone group
- IV digoxin group
- Set designated endpoint criteria following drug administration that were recorded from vital sign flowsheet and uploaded electrocardiograms.
- In addition to baseline characteristics, additional data collected including IV and oral BB, non-DHP CCB, and magnesium doses given prior to and after drug administration were collected
- While initial doses of amiodarone and digoxin varied, majority were in the range of guideline recommendations
- Defined sustained heartrate control as a rate less than 110 beats per minute for longer than 30 minutes.
Inclusion Criteria
- Patients >18 years of age who:
- Had sustained heart rates >120 bpm just prior to drug administration and
- Received a least one dose of BBs or non-DHP CCBs
Exclusion Criteria
- Patients that received a non-study anti-arrhythmic
- Direct cardioversion in the ED
- Treatment with both digoxin and amiodarone
- Prior treatment with amiodarone or digoxin
Outcomes
Primary
- HR control within 12h of amiodarone or digoxin
Secondary
- HR control less than 80 bpm within 12h
- Conversion to normal sinus rhythm (NSR) within 6h and 12h
- HR control within 6h
- Time to HR control and/or conversion to NSR
- Duration of sustained HR control and/or NSR (up to 24h)
Safety
- Bradycardia (HR <60 bpm)
- Hypotension (systolic of 90 mmHg or less)
Results
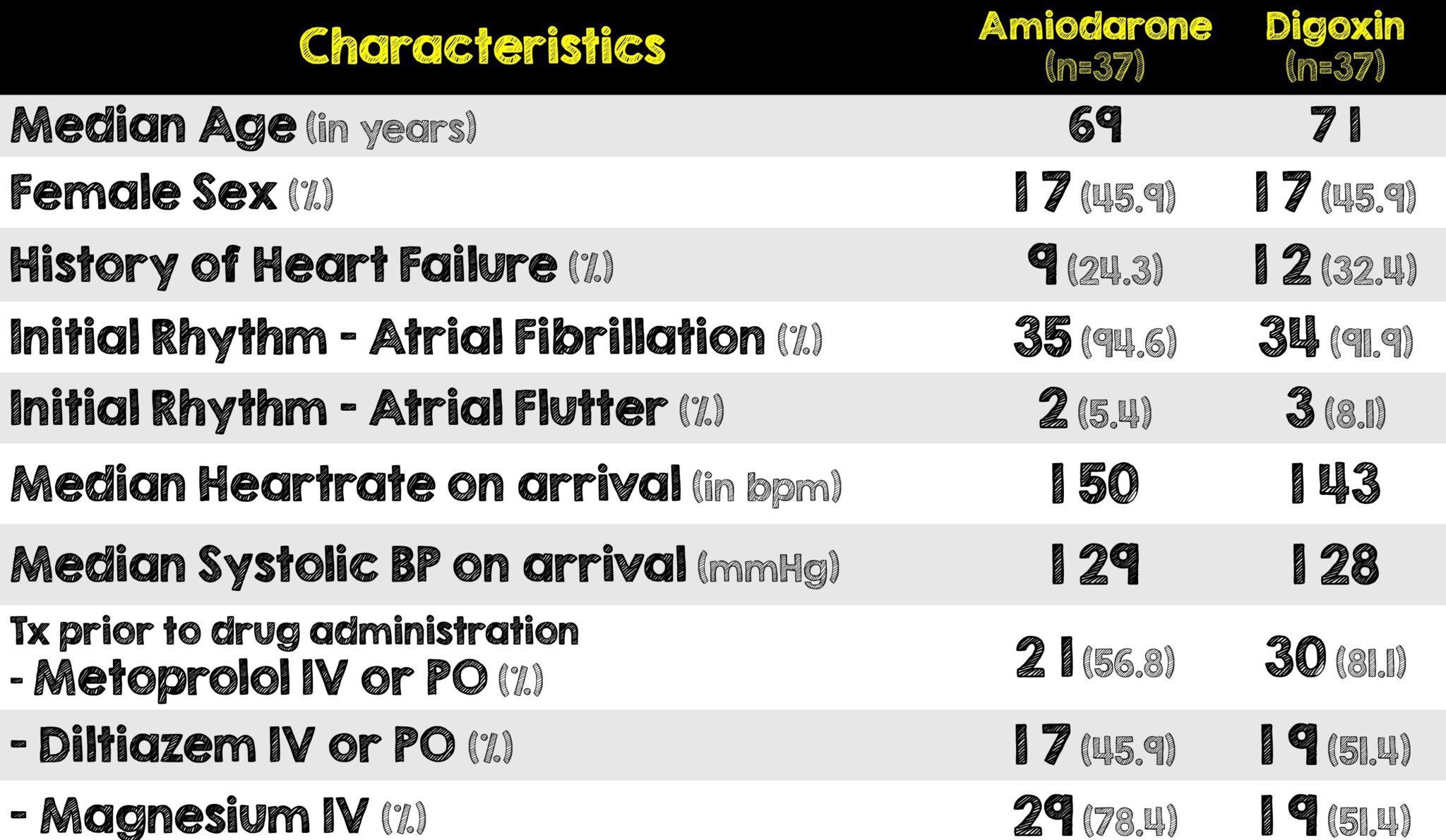
Seventy-Four patients were included in the study
- Amiodarone Group n =34
- Digoxin Group n= 34
Critical Results:
Strengths:
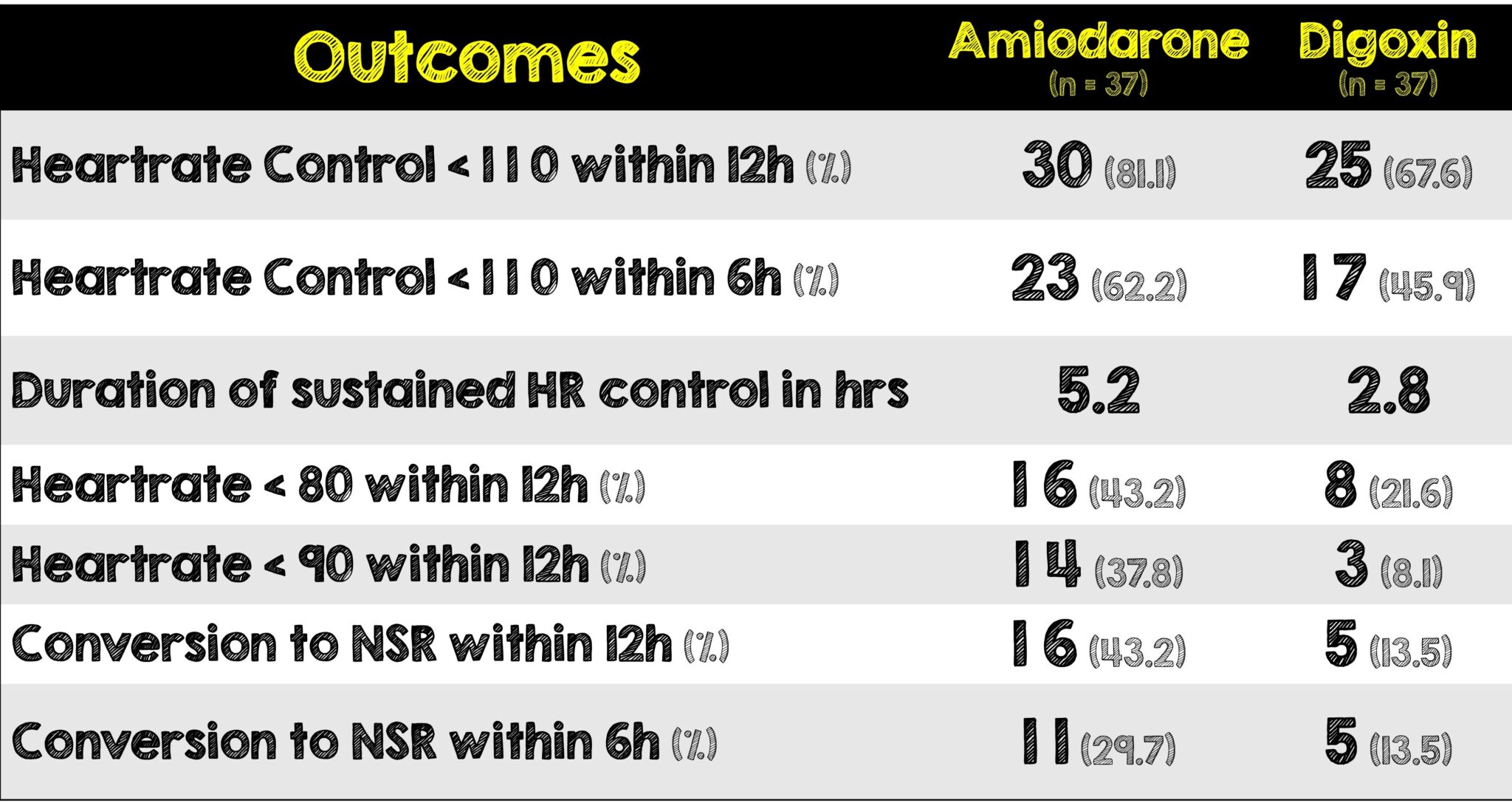
- Amiodarone overall had a greater benefit in HR control for a longer duration of time compared to the IV digoxin group. This is extremely useful in patients with sustained tachycardia refractory to first line therapy.
- The average time to control HR in the IV amiodarone was 1.7h, which is usually the average time for disposition from the ED.
- Average time control HR in the amiodarone group was on par with the study’s average ED length of stay
Limitations:
- Single center, retrospective hospital study may not be able to produce generalizable results.
- Groups were not matched as not many people received IV digoxin
- Exact doses of medications used prior to second line agents were not recorded and thus difficult to determine overall effectiveness and to what degree
- Charting bias may have been introduced as recorded heart rates are dependent on the recorder and the specific time of when heart rate was inputted, rather than standardized data collection.
- Small sample size limits the power of the study and increases margin of error
- A patient-oriented outcome such as mortality was not included
- Follow-up beyond disposition to evaluate hospitalization recurrences related to atrial fibrillation was not included.
Discussion:
- Overall, there was no significant difference in ventricular rate control between IV amiodarone and IV digoxin.
- Higher success towards earlier rate control and longer duration with earlier rhythm conversion was seen in IV amiodarone over IV digoxin, however there were significantly more patients in the amiodarone group would also received IV magnesium. This could have biased the results in favor of amiodarone as we’ve covered this before on REBEL EM before
- The IV amiodarone group required less additional HR control agents to control increased heart rate.
- In terms of safety, hypotension was witnessed from IV amiodarone therefore, avoiding in patients with labile blood pressures may be beneficial.
- These results were corroborated with other another study by Gritensko et al. which also found no significant difference between IV amiodarone or IV digoxin.3
- Another study showed higher treatment failures with (HR< 80-110 bpm) with IV digoxin and time to control faster with IV amiodarone.4
- It’s important to note that the way medications are administered could potentially explain the success (or failure) of rate control. Amiodarone is typically given as a bolus followed by a drip whereas digoxin is given as a loading dose with subsequent doses hours later. The delay in the onset of effect of digoxin could play a role in the poor rate control and overall success in the IV digoxin group.
- Lastly, there is a substantial amount of data missing, specifically the underlying cause of the Atrial Fibrillation with RVR (ie. Sepsis, hyperthyroidism, dehydration, heart failure, ACS, etc). Not having details on how many patients had any of these or whether the groups were balanced skews the interpretation of this study.
Author’s Conclusion
There was no significant difference between amiodarone and digoxin in ventricular rate control of atrial fibrillation with RVR, when used as second-line therapy, after failing AV nodal blocking agents.
Our Conclusion
- Although not statistically significant, trends show amiodarone numerically doing a better job of rate control (HR < 110) at 12 and 6 hours. Several features in this study point to amiodarone being a better agent such as: more patients with heart rate < 80 within 12 hours, rhythm control also within 12 hours, and less additional medications needed within those 12 hours. Unfortunately, without knowing what dose and at what time first line medications were given before second line agents were administered, precludes any definitive conclusions from being made regarding this trial.
Clinical Bottom Line:
- Numerically, amiodarone may be a better medication for rate and rhythm control. Unfortunately, the exact dose and time of administration of first line medications was not reported before a second line medication was given. Therefore, no definitive conclusions can be made about this trial.
References
- Mason JM, et al. Amiodarone versus digoxin for acute rate control of atrial fibrillation in the emergency department. Am J Emerg Med. 2022 Sep 7. Epub ahead of print. PMID: 36115743
- Panchal, Ashish R., et al. “2018 American Heart Association Focused Update on Advanced Cardiovascular Life Support Use of Antiarrhythmic Drugs during and Immediately after Cardiac Arrest: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care.” Circulation, 5 Nov. 2018, PMID: 30571262
- Gritsenko, Diana, et al. “Amiodarone versus Digoxin for Rate Control in Critically Ill Patients with Rapid Atrial Fibrillation or Flutter.” Journal of Emergency and Critical Care Medicine, vol. 2, 2018, pp. 63–63., Link to Paper Here
- Shojaee M, et al. Intravenous Amiodarone versus Digoxin in Atrial Fibrillation Rate Control; a Clinical Trial. Emerg (Tehran). Epub 2017 Jan 10. PMID: 28286836
Guest Post By:

Nileena Johnkutty, DO
PGY-2, Emergency Medicine Resident
RWJBH Community Medical Center, Toms River, NJ
Twitter: @Nileena1023

Mark Ramzy, DO
Emergency Medicine Attending and Critical Care Intensivist
Clinical Assistant Professor of Emergency Medicine
RWJBH Community Medical Center, Toms River, NJ
Twitter: @MRamzyDO
For More Thoughts on This Topic Checkout:
- REBEL EM: LOMAGHI Trial: Magnesium Sulfate for Rapid Atrial Fibrillation
- emDOCs: Management of Atrial Fibrillation: Do’s and Don’ts
Post-Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post Amiodarone Versus Digoxin for Acute Rate Control of Atrial Fibrillation in the Emergency Department appeared first on REBEL EM - Emergency Medicine Blog.