
 I was asked to give a talk at ACEP 2018 on Building the Perfect Curriculum and given 25 minutes to make this happen. As you can imagine there is no way the entirety of building a perfect curriculum can be done in 25 minutes nor is there such a thing as the perfect curriculum, as we are always evaluating and modifying our current curriculum. Therefore the perfect curriculum can always get better. For the sake of this talk however, there are essentially 3 steps to building the perfect curriculum: A needs assessment, optimizing the learning, and evaluation of the curriculum. I opted to focus on optimizing learning. Every year it seems this talk focuses on Kerns 6 step approach to curriculum development, (which is simply one of many models out there) but there is no emphasis on what to do during lectures and weekly conferences.
I was asked to give a talk at ACEP 2018 on Building the Perfect Curriculum and given 25 minutes to make this happen. As you can imagine there is no way the entirety of building a perfect curriculum can be done in 25 minutes nor is there such a thing as the perfect curriculum, as we are always evaluating and modifying our current curriculum. Therefore the perfect curriculum can always get better. For the sake of this talk however, there are essentially 3 steps to building the perfect curriculum: A needs assessment, optimizing the learning, and evaluation of the curriculum. I opted to focus on optimizing learning. Every year it seems this talk focuses on Kerns 6 step approach to curriculum development, (which is simply one of many models out there) but there is no emphasis on what to do during lectures and weekly conferences.
Needs Assessment
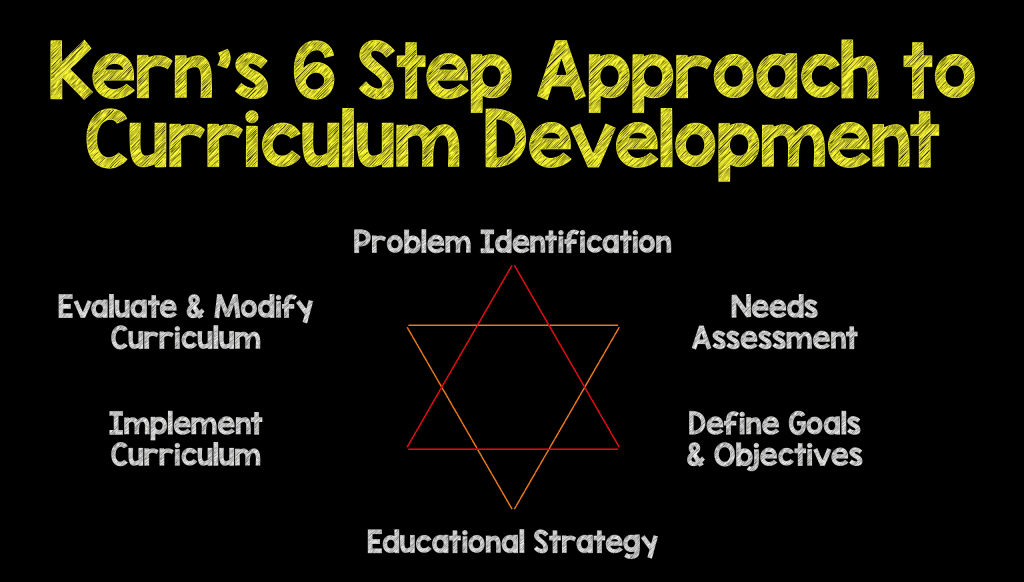
- Kern’s 6 step approach to curriculum development [1] is something any of us can look up.Kern’s model is important in helping us decide what to teach/talk about through needs assessment. This should always be the first step when developing a curriculum
Optimizing Learning
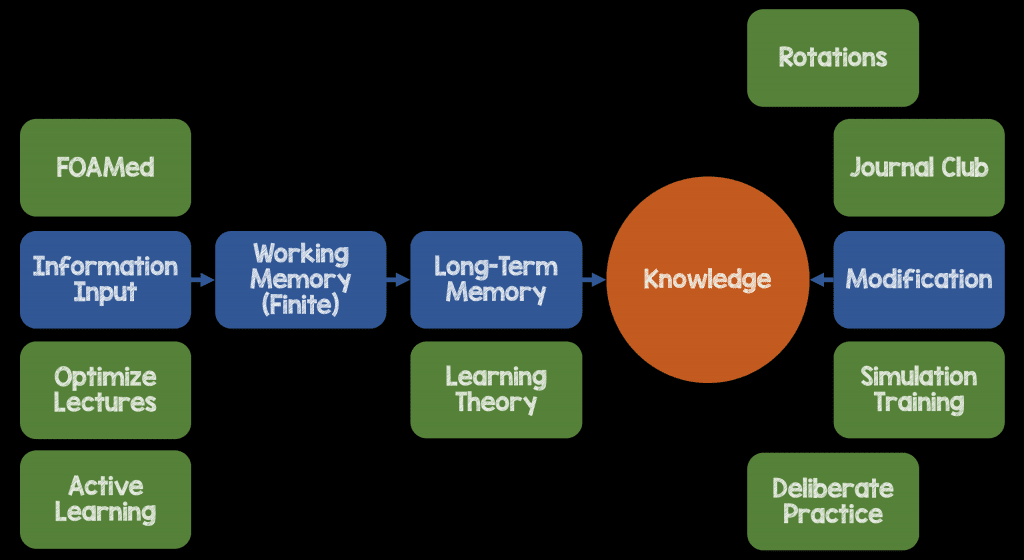
- There are several areas, and this list is not all encompassing, of ways we can optimize learning.
- Optimize Lecture Timing and Multimedia Use to Increase Processing Knowledge
- Active Learning to Increase Interaction in the Classroom
- FOAMed to Solidify Constructs of Nuanced Topics
- Incorporate Learning Theory to Improve Knowledge Retention
- Deliberate Practice to Improve Weaknesses and Continue Learning
- Simulation to Increase Ability to Apply the Classroom to the Clinical Environment
- Journal Club to Learn Critical Appraisal Skills
- Rotations to Learn Physiologies in Different Areas of Medicine
How Our Minds Work
Before we can develop the perfect curriculum we must first understand how our minds work in terms of processing, organizing, and incorporating information from new experiences. For more on this topic checkout this great post on icenetblog.
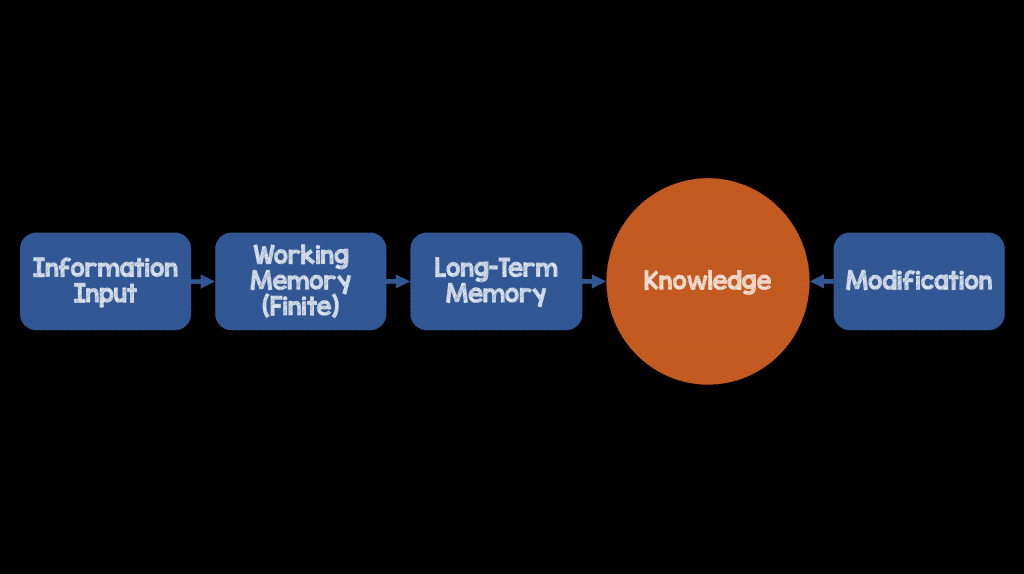
This is a completely oversimplified representation of how new learning occurs and for the rest of my talk I focused on each of these areas using the following construct. Some important points are that several of these areas really belong in several categories, but for simplicity sake, I wanted to create a construct that could be replicated.
Optimizing Lectures
- We need to move away from the traditional 1 hour lecture. This is not optimal for learning. Research has shown that we lose attention after 10 minutes. Obviously we can’t make lectures 10 minutes as this is not ideal, but maybe 20 – 30 minute lectures would be more realistic. 20 – 30 minute lectures allow for a core message and 3 teaching points which is about what anyone can remember from a talk [2].
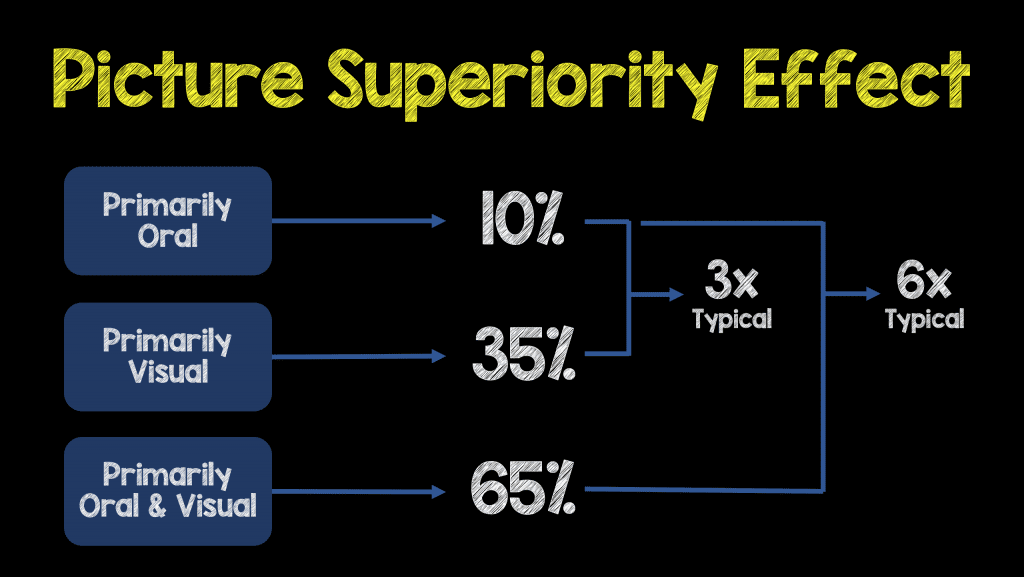
- Pictures are powerful as we associate memories with them. From John Medina’s Brain Rules, a good rule of thumb for knowledge retention is the 10-30-60 rule [3]. We remember best through pictures and not written or spoken words. Increasing videos and images in your presentations can help facilitate just that. Want to describe an ECG that has electrical alternans from a pericardial effusion? Don’t do it with text. Show an ultrasound clip of a heart swinging back and forth and an accompanying ECG that shows electrical alternans.
Active Learning
- Flipped Classroom is where lectures are recorded, or use already created blogs/podcasts, or even articles and shared with learners ahead of time and use classroom time to discuss nuanced topics
- Case Based Learning is another great way to discuss topics during classroom time
- Panel Discussions of controversial topics to show variation in practice are also powerful during classroom time
- Michelle Lin at ALiEM has a great series called the IDEA series, which are educational innovations related to resident education, and a very useful resource in accomplishing active learning during classroom time
FOAMed
- Personal Learning Networks: Interaction with others in different environments helps solidify constructs of nuanced topics
- Podcasts/Blogs: Have faculty identify podcasts/blogs that would help reiterate or discuss topics being covered in respective blocks of curriculum
Learning Theory [4]
- Retrieval Practice: Focuses on getting information out of students minds instead of dumping information in (i.e. low stakes quizzes)
- Spaced Repetition: Teach concepts in the classroom and then put out reminders after the fact to help with memory and retention of information. A new concept is discussed in conference, maybe spend 20 minutes reviewing what was covered from the prior weeks conference, then use a FOAM resource at a later date to reiterate what was discussed, and finally maybe a monthly summary of topics discussed to help jog the residents memory.
- Interleaving: Mixing up topics (varied practice) instead of blocking into the same content.Interleaving improves mastery and long term retention. This helps improve learners ability to transfer learning from one situation and apply it successfully to another (i.e. all chest pain patients don’t come in with ACS). Life’s problems and opportunities come at us unpredictably and out of sequence. Interleaving teaches us critical thinking (assess context and discriminate between problems)
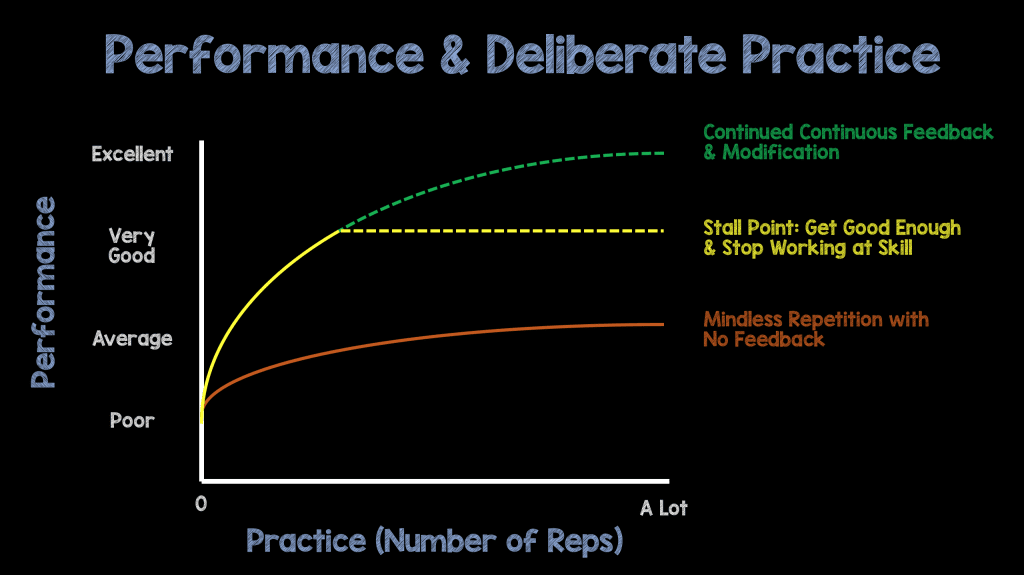
Deliberate Practice
- If I were to ask you, who is the greatest male tennis player in the world, you would say Roger Federer. He didn’t become the best through simply practicing over and over. He has a coach that gives him continuous feedback.
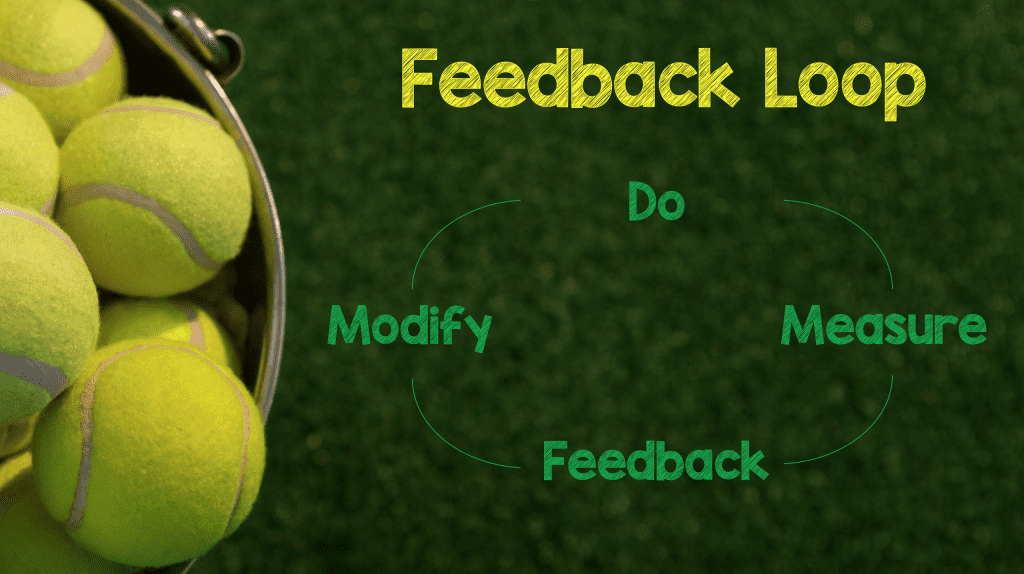
The Feedback Loop: Do an Activity –> Set Clear Learning Goals to Measure –> Give Feedback –> Modify/Refine Your Activity Based on Feedback
The 10,000 Hours of Practice to Gain Expertise is Bogus. We need continuous feedback and modification to gain expertise [5]
- Low Stakes Assessment: This is important to help increase competence (What areas am I weak in) NOT confirm current competence. Question banks are a great way to discuss topics during classroom time (i.e. Rosh Review, PEER Review)
- Procedure Workshops: Breaking up procedures into microskills and going through each step of the process with real time feedback to improve procedure technique is also another way to accomplish.
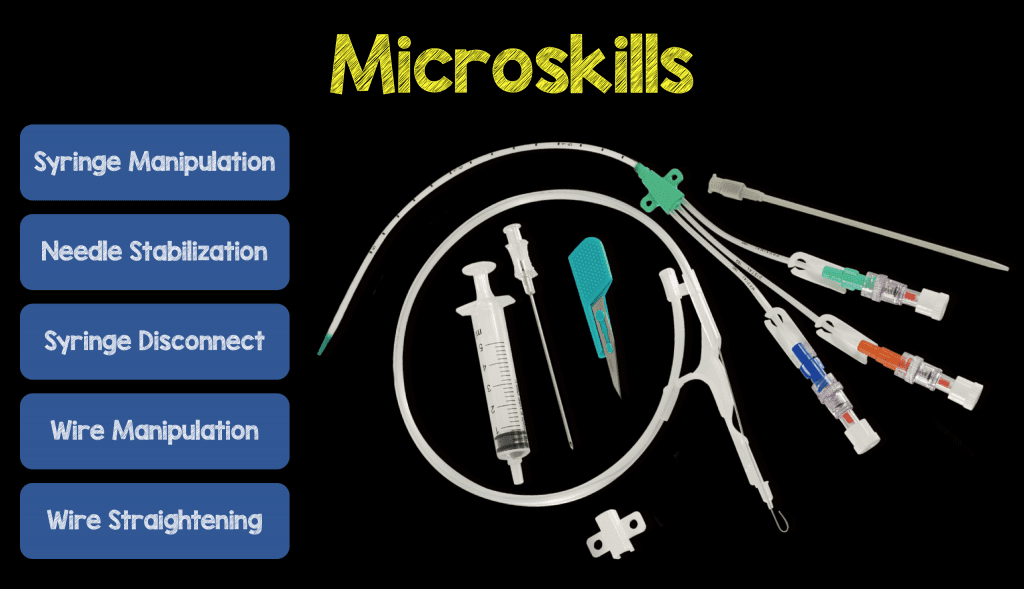
An example of microskills with central line placement
Simulation Training
- This gives learners the ability to apply what they learned in the classroom and apply it in the clinical environment
- Helps emphasize the importance of teamwork. Let’s face it, care of any patient in the ED is a team sport
- Also emphasizes the importance of clear, effective, closed loop communication
Journal Club
- Emphasis on critical appraisal of literature, evidence-based medicine and how to translate research to application at the bedside
Rotations
- Pick rotations that will help residents learn physiology of disease and management of disease outside the ED
Evaluation of Curriculum
- Assessment of curricula on a quarterly, bi-annual, and annual time frame is essential to ensure what you are doing to optimize learning is working and there are no gaps in knowledge learning. The exact time to do this will vary depending on the program and what is available
There are so many ways to help optimize learning in academia, above is a list of some of the ways, and again, not all encompassing, that I think we can help our learners optimize their learning. All thoughts, feedback, and other suggestions are always welcome, as this is always a moving target.
References:
- Kern DE et al. Curriculum Development for Medical Education: A Six Step Approach. 2009 [Link HERE]
- Schmidt HG et al. On the Use and Misuse of Lectures in Higher Education. Health Professions Education 2015. [Link HERE]
- Medina J. Brain Rules. 2014 [Link HERE]
- Brown PC et al. Make it Stick: the Science of Successful Learning. 2014. [Link HERE]
- Ericsoon KA. Deliberate Practice and the Acquisition and Maintenance of Performance in Medicine and Related Domains. Acad Med 2004. PMID: 15383395
Post Peer Reviewed By: Jeff Riddell (Twitter: @Jeff__Riddell)
The post Building the “Perfect” Curriculum appeared first on REBEL EM - Emergency Medicine Blog.