
 Background: Low back pain is an extremely common presentation to US Emergency Departments (EDs) representing 2.4% or 2.7 million visits annually. The vast majority of presentations are benign in etiology but can be time consuming and frustrating for both patients and physicians. For patients, most will have persistent symptoms a week after presentation and many will have continued functional impairment months after symptom onset. Physician frustrations are multifaceted – preoccupation for finding the rare dangerous back pain patient (the one with an epidural abscess or vertebral osteomyelitis), difficulty in relieving pain and concern for secondary gain (i.e. opiate abuse or diversion). Post-ED analgesia regimens range from NSAIDs and acetaminophen to muscle relaxants (i.e. cyclobenzaprine) to benzodiazepines and opiates. Previous work from this group demonstrated a lack of benefit for adjunct cyclobenzaprine or oxycodone/acetaminophen to naproxen. Now, they turn their eye to the use of diazepam in addition to naproxen.
Background: Low back pain is an extremely common presentation to US Emergency Departments (EDs) representing 2.4% or 2.7 million visits annually. The vast majority of presentations are benign in etiology but can be time consuming and frustrating for both patients and physicians. For patients, most will have persistent symptoms a week after presentation and many will have continued functional impairment months after symptom onset. Physician frustrations are multifaceted – preoccupation for finding the rare dangerous back pain patient (the one with an epidural abscess or vertebral osteomyelitis), difficulty in relieving pain and concern for secondary gain (i.e. opiate abuse or diversion). Post-ED analgesia regimens range from NSAIDs and acetaminophen to muscle relaxants (i.e. cyclobenzaprine) to benzodiazepines and opiates. Previous work from this group demonstrated a lack of benefit for adjunct cyclobenzaprine or oxycodone/acetaminophen to naproxen. Now, they turn their eye to the use of diazepam in addition to naproxen.
Article:Friedman BW et al. Diazepam is no Better Than Placebo When Added to Naproxen for Acute Low Back Pain. Ann Emerg Med 2017. PMID: 28187918
Clinical Question: Does the addition of diazepam to naproxen in patients presenting with acute, nontraumatic, nonradicular low back pain improve functional outcomes at 1 week?
Population: Adults aged 21 to 69 years of age who presented to a single urban ED for the management of acute low back pain (lower border of the scapula to the upper gluteal folds). Patients had to have functionally impairing back pain (score > 5 on the Roland-Morris Disability Questionnaire (RMDQ)) and had to be discharged home.
Intervention: Naproxen 500 mg PO Q12 PRN pain + diazepam 5-10 mg PO Q12 PRN pain
Control: Naproxen 500 mg PO Q12 PRN pain + 1-2 placebo pills Q12 PRN pain
Outcomes:
- Primary: Improvement in the RMDQ score between ED discharge and 1 week follow-up.
- Secondary: Pain intensity at 1 week and 3 months measured on a 4-point descriptive scale.
Design: Prospective, randomized, double-blind, placebo-controlled comparative efficacy study
Excluded: Presence of radicular pain, pain greater than 2 weeks in duration, baseline low back pain frequency of once per month or more, presence of a nonmusculoskeletal cause of back pain (i.e. pyelonephritis), patients with direct trauma, pregnancy or breast feeding, chronic fatigue syndrome and those unavailable for follow-up.
Primary Results:
-
545 patients screened for enrollment
- 114 patients included based on inclusion criteria
- No significant difference in baseline demographic characteristics between the two groups
- 112/114 patients (98%) were followed up at 1 week
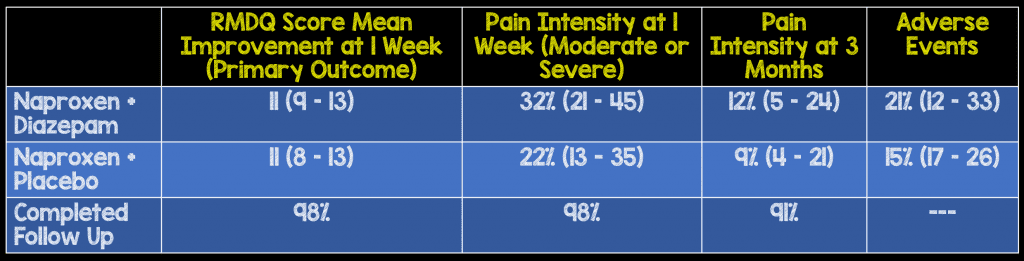
Critical Findings (95% CI)
Strengths:
- Study asked a simple, clinically relevant question with a patient centered outcome
- Randomization and blinding were appropriately performed
- The functional assessment tool (RMDQ) has been previously validated
- All study medications were supplied prior to discharge (no question of whether prescriptions were filled or went unfilled)
- Dosing was designed to avoid side effects where possible and use the minimum necessary dose while allowing for up-titration if necessary
- All patients were given a 10-min educational intervention on back pain prior to discharge
- Follow up was near complete at 1 week and remained excellent at 3 months
Limitations:
- While the study sought to include a broad representation of patients with musculoskeletal back pain, almost 80% of patients approached were excluded prior to enrollment
- The study was conducted in a single urban hospital. This limits generalizability
- Many of the inclusion/exclusion criteria are susceptible to recall bias (i.e. pain greater than 2 weeks)
- The presence of radicular pain led to exclusion but this can be quite subjective. There was no mention of inter-rater reliability for this criteria
- Unemployment, a known factor involved in recovery from back pain, was more common in the naproxen + diazepam group (19% vs. 5%)
- Although use of medication was asked at 1 week and 3 months follow up, it is difficult, if not impossible, to know if the reported use was accurate
- There is no mention of medications used in the ED for back pain prior to discharge. Additionally, it’s unclear how this would have affected outcomes.
Authors Conclusions:
“Among ED patients with acute, nontraumatic, nonradicular low back pain, naproxen + diazepam did not improve functional outcomes or pain compared with naproxen + placebo 1 week and 3 months after ED discharge.”
Our Conclusions:
In this single center study, the addition of diazepam to naproxen did not improve functional outcomes in patients presenting with acute nontraumatic, nonradicular low back pain.
Potential to Impact Current Practice:
Based on the best available data, it does not appear that diazepam should be routinely added to an NSAID for outpatient management of acute, nontraumatic low back pain.
Clinical Bottom Line:
The addition of diazepam to naproxen does not appear to improve acute nontraumatic low back pain outcomes. While side effects were not significantly increased, the absence of benefit should limit this practice. Further multi-center data validating these results would be helpful.
Checkout More on This Topic at:
Core EM: Treatment of Acute, Non-Traumatic Low Back Pain
Post Peer Reviewed By: Salim Rezaie (Twitter: @srrezaie)
The post Effectiveness of Diazepam Adjunct Therapy in Acute Low Back Pain appeared first on REBEL EM - Emergency Medicine Blog.