
Radiology teaching during medical school is variable, ranging from informal teaching to required clerkships.1 Many of us likely received an approach to a chest x-ray, but approaches to other studies may or may not have not been taught. We can do better! Enter EMRad, a series aimed at providing approaches and improving interpretation of commonly ordered radiology studies in the emergency department. When applicable, it will provide pertinent measurements specific to management, and offer a framework for when to get an additional view, if appropriate. To begin: the elbow.
Learning Objectives
- Interpret elbow x-rays using a standard approach
- Identify clinical scenarios in which an additional view might improve pathology diagnosis
Why the elbow matters and the radiology rule of 2’s
The Elbow
- Approximately 2-3% of all ED visits involve the elbow.2
- Missed elbow injuries can be highly morbid.
Before we begin: Make sure to employ the rule of 2’s3
- 2 views: One view is never enough.
- 2 abnormalities: If you see one abnormality, look for another.
- 2 joints: Image above and below the injury (especially for forearm and leg).
- 2 sides: If unsure regarding a potential pathologic finding, compare it to another side.
- 2 occasions: Always compare with old x-rays if available.
- 2 visits: Bring the patient back for repeat films.
An approach to the traumatic adult elbow x-ray
- Adequacy/Alignment
- Effusions or fat pads
- Bones
- Consider an additional view
1. Adequacy/Alignment
-
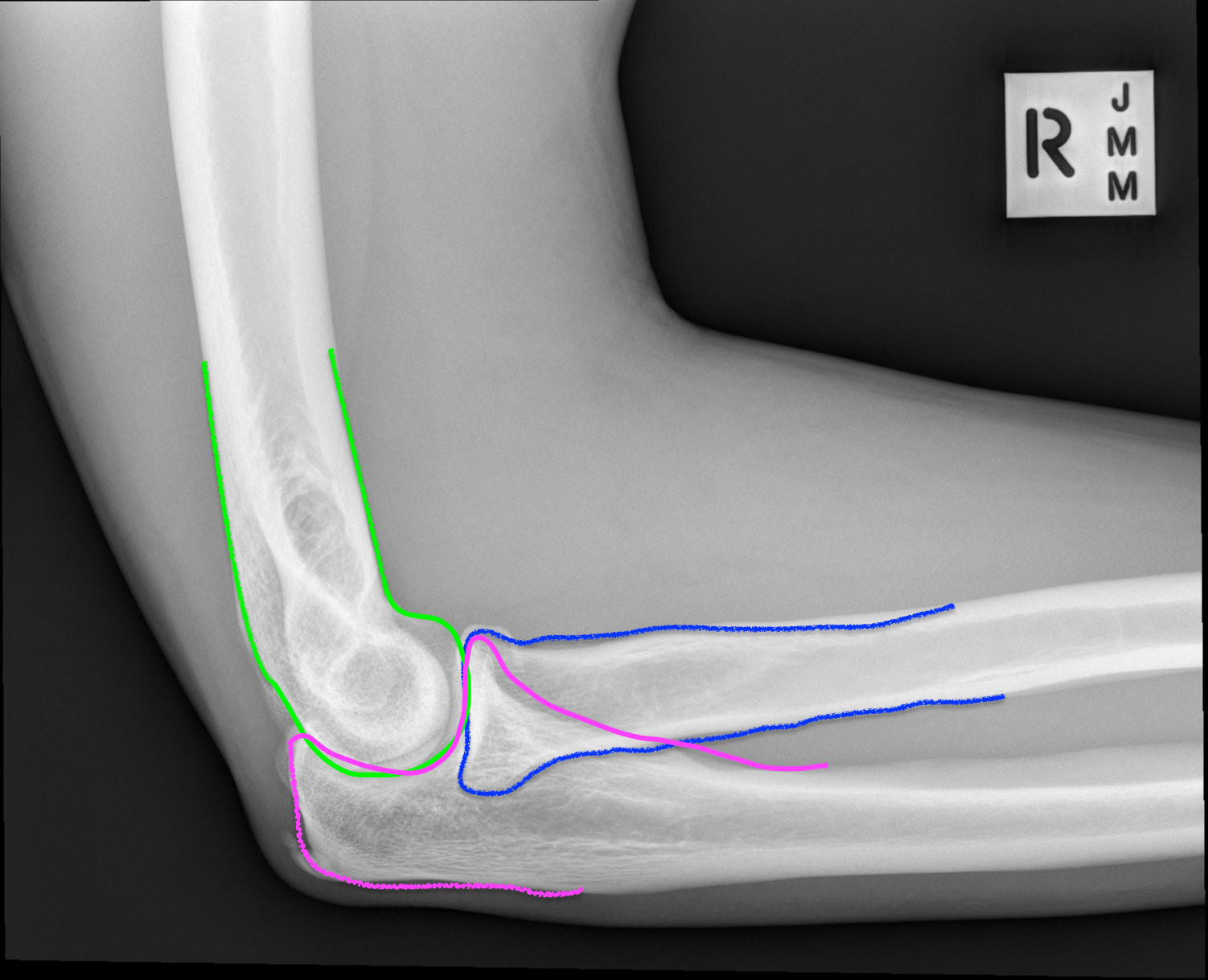
Lateral View
- Check for a “Figure of 8” to ensure that this is a true lateral view.

-
Anterior humeral line
- A line drawn along the anterior aspect of the humerus should intersect the middle ⅓ of the capitellum.
- If it does not, consider distal humerus fracture.
-
Radiocapitellar line
- A line drawn along the middle of the radius should intersect the capitellum.
- If not, consider radial head dislocation or subluxation.

2. Check for effusions or fat pads
Lateral View
- An anterior fat pad can be normal but if excessive or “sail sign” think radial head fracture in adults
- An posterior fat pad is always pathologic. In adults, this indicates intra-articular trauma.

How do you know when too much is too much? The normal anterior fat pad is typically parallel to the humerus, usually angulated ≤15 degrees from the humeral shaft. When there is a significant effusion, it appears more angulated or like a sail, hence a “Sail Sign.”4
3. Bones
- Trace the bone cortex carefully on both AP and lateral views.
- Pay close attention to all aspects of the humerus, radius, olecranon.

4. Consider an additional view
External Oblique View
- When: Sometimes included as the 3rd view in a series
- Why: This is better at seeing the radial head. Consider obtaining this view if there is a high suspicion for radial head fracture.

Coyles View
- When: High index of suspicion for radial head fracture

Learn More
- Find an abnormality and not sure which splint to apply? Read more about this in our SplintER Series: Common ED Splint Techniques.
- Afraid you might miss something commonly missed or catastrophic? Read more at “Can’t Miss” Elbow Injuries.
- Want a more in-depth approach to elbow radiography? Take a radiology master class or check out Radiopaedia’s approach.
References:
-
1.Schiller P, Phillips A, Straus C. Radiology Education in Medical School and Residency: The Views and Needs of Program Directors. Acad Radiol. 2018;25(10):1333-1343. https://www.ncbi.nlm.nih.gov/pubmed/29748045.
-
2.Goldflam K. Evaluation and treatment of the elbow and forearm injuries in the emergency department. Emerg Med Clin North Am. 2015;33(2):409-421. https://www.ncbi.nlm.nih.gov/pubmed/25892729.
-
3.Chan O. Introduction: ABCs and Rules of 2. In: ABC of Emergency Radiology. John wiley & Sons, Ltd; 2013:1-10.
-
4.Blumberg S, Kunkov S, Crain E, Goldman H. The predictive value of a normal radiographic anterior fat pad sign following elbow trauma in children. Pediatr Emerg Care. 2011;27(7):596-600. https://www.ncbi.nlm.nih.gov/pubmed/21712751.
Author information

The post EMRad: Radiologic Approach to the Traumatic Elbow appeared first on ALiEM.