
 As EM physicians, we are taught how to manage and treat many serious and life threatening conditions, most of them we know like the back of our hands, and some we look up on shift. The most important things to know are the “think on your feet” situations, when patients are actively trying to die in front of you, and you don’t have the time to look things up. We all know how to manage a bleed, whether internal or external, but do you know how to treat bleeding in a Hemophilia patient?! I didn’t until April, 2018 when my newborn son was diagnosed with Hemophilia A.
As EM physicians, we are taught how to manage and treat many serious and life threatening conditions, most of them we know like the back of our hands, and some we look up on shift. The most important things to know are the “think on your feet” situations, when patients are actively trying to die in front of you, and you don’t have the time to look things up. We all know how to manage a bleed, whether internal or external, but do you know how to treat bleeding in a Hemophilia patient?! I didn’t until April, 2018 when my newborn son was diagnosed with Hemophilia A.
In this segment, I will explain and simplify hemophilia for you down to the “need to know” essential information so when you are managing a hemophilia patient in the ED, like my son, you will know what to do.
Basics: The Clot
- Blood needs to clot. It needs to plug the hole so it doesn’t leak out of the hose!
- When endothelial injury occurs this activates the clotting cascade (extrinsic and intrinsic)
- Think of the extrinsic pathway as the “quick fix”, like putting duct tape on the hole. It occurs faster, but is less stable. This is fibrin mesh formation and platelet aggregation. You still need the intrinsic pathway to keep going in order to form the more robust clot that will permanently plug that hole. Clotting factors help support the plug.
- When clot formation is working the way it is supposed to, we form an immediate plug, followed by a delayed more secure clot.
- Both of them lead to activation of factor X (the common pathway)
- The intrinsic pathway has a bunch of clotting factors, one activates the other, like dominoes falling. If one of the Domino pieces are missing, the cascade can’t go on, and no “robust” clot will form.
-
Intrinsic pathway deficiences
- If factor VIII is missing = Hemophilia A
- If factor IX is missing = Hemophilia B
- If factor XI is missing = Hemophilia C (rare)
- aPTT measures the intrinsic pathway. While PT/ INR measures the extrinsic pathway
Who Gets It:
- X-linked recessive disorder. The offspring who inherits this affected X chromosome gets the disease
- Primarily affects Males since they have one X and one Y, but female carriers (XX) can exhibit the disease if the affected X is being expressed
-
Categorized by severity into severe, moderate or mild based on the available factor in their blood. The less available, the more severe the disease.
- Severe: <1% of factor is available
- Moderate : Between 1 and 5 % available factor in their blood
- Mild: More than 5% factor available
- Severe hemophiliacs are usually on home prophylaxis. They infuse their factor replacement at home 2-3 times a week either through a port, or IV.
Hemophilia in Your ED
-
- Kids or adults who have hemophilia are very well educated about their condition. Listen to them
- All the guidelines you know about pediatric or adult head trauma, fractures, etc go out the window. They do not apply to patients with hemophilia.
- These patients can have life-threatening bleeds spontaneously, or due to minor trauma.
- These patients are able to manage their minor issues at home so when they come to the ED, they are usually in trouble.
- If you, or the patient or the parents suspect a bleed, immediately infuse factor replacement regardless if they took their home prophylaxis dose or not. You treat based on suspicion of a possible bleed, NOT the confirmation of one.
- The treatment is to replete the missing factor. There are many types/ brands of factor repletion, some are recombinant (most common), some are human derived. Try to use what the patient uses at home, or has used before. Most patients will actually bring their factor with them to the ED (If they don’t use what you have at your facility).
-
Factor replacement is based on how severe the bleed is
- Full dose factor repletion: in major bleeds (CNS, GI, neck/throat, major trauma)
- Half dose factor repletion: in minor bleeds (superficial cuts, mucous membrane bleeds, epistaxis, soft tissue, muscle, mild hemarthrosis)
- When in doubt go big. Give full factor repletion. The extra factor will not cause adverse effects, the body will simply eliminate it later.
- Beware of hidden bleeds.
-
-
- Spontaneous intracranial hemorrhage: can present with headache or vomiting
- Retroperitoneal/ psoas bleed: presents with vague groin pain, abdominal pain, or back pain, as well as paresthesia in the medial thigh.The hip will be flexed and internally rotated. Pain with hip extension. Retroperitoneal bleeds can cause hypovolemic shock.
- Muscle hematomas : check glutes, and thighs.
- Have a low threshold to treat
-
How to Replete Factor:
Regardless of their severity level, or if they took their home prophylaxis, in the ED the full dose repletion for
- Factor 8: 50 U/kg. Each U/kg = an increase of factor by 2%
- Factor 9: 100 U/kg .Each U/kg = an increase of factor by 1%
If you want to give half dose repletion, for the minor bleeds, just give half that dose.
Remember, it is always better to overtreat than undertreat.
Other Meds you can Use
-
If you do not have factor replacement in your facility you may use
- Activated PCC (FEIBA) = 80-100U/kg
- Recombinant factor 7a= 90 mcg/kg
-
If those also are not available you may use:
-
Cryoprecipitate
- 80 – 100U of factor VIII per single donor bag; Used if factor VIII concentrates are not available
-
FFP
- 1U of factor VIII per mL of FFP (1U FFP raises the factor level by only 3 to 5%); Volume overload is a limiting factor
- You will need a lot of volume to achieve the units needed, you will probably overload your patient before you reach therapeutic doses.
-
Cryoprecipitate
- Other adjuncts you can use:
These will help but should not replace factor infusion. They are used as adjuncts in minor cuts and mucosal bleeds
-
DDAVP
- releases Von Willebrand factor from endothelium, VwF is attached to factor 8, so essentially you release more factor 8 into the circulation
- Can increase factor VIII by 3x – 5x (onset 30min; peak 90 to 100min)
- Dose: 0.3mcg/kg/dose IV
-
TXA (stabilizes the fibrin by blocking fibrinolysis)
- Dose is 10-15 mg/kg IV
-
Aminocaproic acid (stabilizes the fibrin by blocking fibrinolysis).
- dose is 50-100 mg/Kg q 6 hours PO not to exceed 6 gms per dose or 24 gms in 24 hours.
-
In mouth bleeds you may use
- Amicar mouthwash: may crush tablet and mix with water, use elixir or IV preparation 2.5 mg/10 ml
Or
-
-
- Swish 10 ml over site gently for 2 minutes, repeat QID, then NPO for 1 hour
-
The Workup:
Once you obtain the IV, draw labs that will help the hematologist. Like factor 8, or 9 level pre infusion, and one hour after infusion of replacement. Some will ask to send inhibitor levels (explained below)
Depending on the presentation, you should obtain appropriate imaging. Head CT, accelerated head MRI (in some centers), abdominal CT, x-rays or any other imaging should be done, but AFTER giving factor repletion. Do not delay factor infusion for imaging or labs.
Those with Inhibitors:
Some patients (30% of hemophilia A and 5% of hemophilia B) develop antibodies against replaced and natural factor 8 or 9. This usually occurs with the first 50 infusions of factor, and also has a genetic predisposition. It is measured in Bethesda units (BU).
Essentially if a patient has a lot of inhibitors (i.e antibodies against the factor) it makes things much harder:
- Giving them factor replacement won’t work because of the antibodies they have in their system (the inhibitors)
- Inhibitors against factor 9 can actually cause anaphylaxis
- It increases severity. So if a patient with mild hemophilia develops inhibitors, they are considered severe now because inhibitors will also attack native factor
To determine if someone has developed inhibitors the lab can perform clotting factor mixing test
- mix normal plasma with patients serum
- Normal = aPTT will normalize
- Inhibitor = aPTT remains prolonged
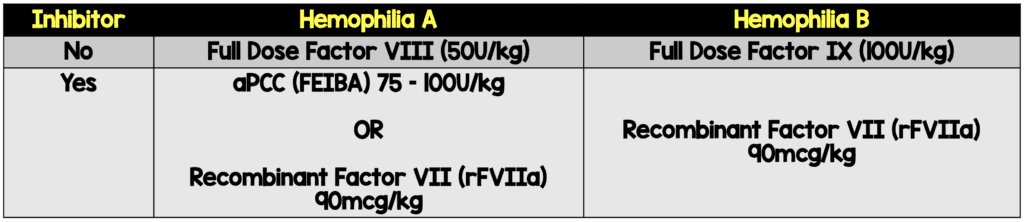
Treating Hemophilia who has Inhibitors:
- If the patient develops a small amount of inhibitors (Low titers ≤5BU) you can still treat with factor concentrates, if high titers of inhibitors are present (>5BU) may require treatment with factor VIIa concentrates or aPCCs.
For simplicity, if a patient tells you they have inhibitors, don’t bother with factor replacement just give:
- FEIBA (Factor Eight Inhibitor Bypass Activity) which is aPCC (activated prothrombin complex concentrate) contains non-activated factors II, IX, and X, proteins that make up the prothrombin complex, and active factor VII. Care should be taken in Hemophilia B with inhibitors as they can have anaphylactic reaction to FEIBA because it contains factor IX.
OR
- Recombinant activated factor VII (rFVIIa).
Dosing:
- Activated PCC (FEIBA) = 80-100U/kg
- Recombinant factor 7a = 90 mcg/kg
Hemlibra (Emicizumab)
- An antibody that works as factor VIII. It tricks your body into completing the cascade as if factor 8 was there. But it is not actually a factor.
- Used as prophylaxis for those who have inhibitors, and also (as of recently) those with no inhibitors
- If patients are on this medication, you STILL give them factor replacement at full doses if they get injured. Nothing changes.
- If a patient is on Hemlibra, DO NOT give FEIBA. It can cause thrombotic events.
Acquired Hemophilia
- These are patients who develop inhibitors to clotting factors, usually in adults.
- Causes: Malignancies, Pregnancy, Autoimmune Disorders, Idiopathic
- If an adult patient presents with unexplained isolated PTT elevation,with normal PT and platelets, think of acquired hemophilia.
- It can be devastating, and has a high mortality.
Non-Bleed Related Visits
The haemophilia patient may present to the emergency department for non trauma related reasons. Keep the following points in mind:
- If they are febrile make sure they don’t have a central-line infection. Some of these patients have ports
- Avoid giving them aspirin or NSAIDs, this will increase the risk of bleeding
- Avoid IM injections. They can cause hematomas.
- Avoid procedures like arterial lines, lumbar punctures, or arthrocentesis. If they are necessary then replete factor first.
Take Home Pearls:
- Infuse factor first, investigate later
- Treat when bleeding is suspected, not confirmed. Have a low threshold!
-
It is better to over treat than undertreat. Give full dose when in doubt
- Factor 8 = 50U/kg
- Factor 9 = 100 U/kg
- Beware of hidden bleeds (brain, RP, deep muscles)
-
If patient has inhibitors, or no factor available you may use
- Activated PCC (FEIBA) = 80 -100U/kg
- Recombinant factor 7a = 90 mcg/kg
For More on This Topic Checkout:
- REBEL EM: Hemophilia – What’s so Bloody Funny?
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post Hemophilia: For the Love of Bleeding appeared first on REBEL EM - Emergency Medicine Blog.