Chest Pain (CP) is a very common complaint seen in emergency departments around the world. In the US specifically anywhere from 8 – 10 million patients present to the ED complaining of CP. Many use liberal testing strategies to prevent missing acute coronary syndrome (ACS) or other major adverse cardiac events (MACE), but this is not without increase in healthcare cost and false positive testing leading to more downstream testing. In recent years there have been several diagnostic protocols developed to help determine a portion of these patients as low risk to facilitate early discharge, prevent this over testing, while still having a >99% NPV for MACE at 30 days.
Disclaimer: To be clear, this is the way I manage low risk chest pain and certainly there is more than one way, but I think at the current time in the US, this is the best we have. Also, at the time of this post being written, we DO NOT have high sensitivity troponins in the US.
What does twitter say is an acceptable miss rate for MACE (Myocardial Infarction, CABG, Heart Catheterization, and/or Death)?
For those people who voted for 0%, there really isn’t anything in medicine that is 100%. If we are getting to a 0% miss rate then we are way over testing our patients via increased downstream testing. I think it is important to keep evidence based medicine (EBM) in mind as we decide which patients are low risk and which ones aren’t. EBM is defined as:
- Clinical Judgment
- Relevant Scientific Evidence
- Patient Values and Preferences
Lets Start with the TIMI Risk Score
- TIMI was not derived for an undifferentiated chest pain population in an ED setting. Instead it was derived for patients who were already high risk to see if they would benefit from early invasive therapies. Using TIMI to determine low risk CP is like using a hammer to put a screw in. It is a tool, but this is not what the tool was intended for.
- TIMI is binary. In other words it is yes or no. Did you take aspirin the last 7 days…yes or no? Thats an easy one. What about did you have recent (≤24hrs) severe angina…yes or no? This is such a subjective component of the TIMI Score and if you have ever taken care of a patient with CP you know that the story is not always black and white. Sometimes it is grey, but TIMI forces you to say yes or no.
- TIMI = 0. All of the accelerated diagnostic protocols (ADPs) evaluated a TIMI score of 0 to achieve a >99% NPV for MACE.
- Issue Number One: None of these trials were done in the US and therefore not a US population.
- Issue Number Two: A TIMI Score of 0 only identified 10 – 20% of patients as low risk in these studies
- ASPECT (2011) = 9.8% low risk [1]
- New Improved ADP (2012) = 12.3% low risk [2]
- ADAPT (2012) = 20% low risk [3]
- What about TIMI vs HEART Score to determine low risk patients?
- Sun B et al. Circulation 2015: 8,255 patients –> Receiving Operator Characteristic (ROC) Curve = HEART 0.75 vs TIMI 0.68 [4]
- Backus et al Current Cardiology Reviews 2011 –> c-statistic = HEART 0.9 vs TIMI 0.65 [5]
- The HEART Score is more accurate than TIMI and specifically outperforms TIMI at “low risk” thresholds
Now Lets Talk About the HEART Score
A HEART Score of 0 – 3 is considered low risk, but there are some very important caveats to this:
- Positive Troponin: It is possible to have an elevated troponin level and have everything else be negative on the HEART Score. Technically, this would still be a low risk HEART Score, but a positive troponin in my mind is not low risk.
- Dynamic ECG Changes: You could also potentially only have ECG changes and everything else be negative on your HEART Score. Again, this would be a low risk HEART Score. However, if there are old ECGs for comparison or you get repeat ECGs and there is dynamic change, this again is not low risk despite the score
- Risk Factors: If a patient doesn’t go to the doctor then patient won’t have medical problems. This is an issue with both the TIMI and HEART Scores. The patient will say they don’t have medical problems when in fact they do, this will falsely lower your risk stratification score and this should be taken with a grain of salt in evaluation of patients.
- So minus the above caveats, how good is a HEART Score of 0 – 3 at predicting 30 – 45 day MACE?
- 17 Trials with >25,000 patients
- Almost 40% identified as low risk
- 30 – 45d MACE Rate = 1.6%
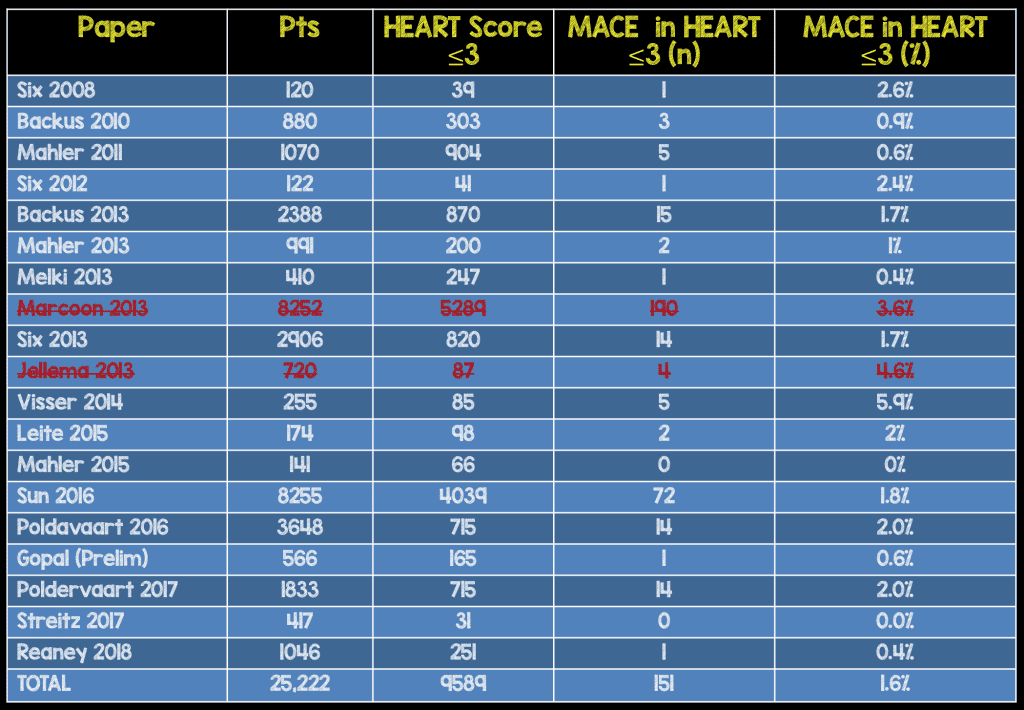
*Addendum (02/19/2016): Since writing the original blog post, I received a very nice email from one of the original creators of the HEART Score, Barbra Backus. She had some issues with the Marcoon and Jellema papers that I think are very reasonable and also mentioned a new publication of the HEART Score just published (Sun et al 2016).
*Addendum (08/15/2018): Received an email from Ben Mati, MD at Ventura County Medical Center was working on his grand rounds talk on low risk chest pain and added a few more studies to make this table more current.
- Jellema 2013: The results of the entire population of HEART Score 0 – 3 were not included in this manuscript making it hard to know what the exact MACE rate was in this population. There was a subcohort of patients that were admitted to the hospital, for a second troponin test, that were included. Using this population creates a huge selection bias in that although these patients were HEART Scores of 0 – 3, they were admitted because they were thought to be higher risk.
-
Marcoon 2013: The definitions of patient history and ECG used in Marcoon’s paper are different than the original HEART Score definitions.
- History: Patients with 2 elements typical for ACS (oppressive, burning, left sided, substernal chest pain, radiation, diaphoresis, vomiting, short of breath) were scored as atypical instead of intermediate/suspicious and patients with 3-4 elements typical for ACS were scored as intermediate instead of highly suspicious.
- ECG: Only ECGs showing ST elevations were scored as a 2, while t-wave inversions/ST depression were scored as a 1, and nonspecific changes were scored as a 0. Again these definitions would result in underscoring of the ECGs.
- Combining these two issues, you can see patients who were scored as low risk HEART scores, may not in fact have been low risk.
- Sun 2016: This was just published and adds another >8,000 patients to our external validation of the HEART Score [7].
Can We do Better than 1.6% MACE?
I think we can. Mahler et al have published 2 external validation studies of the HEART Score in the US using a HEART Score of 0 – 3 + contemporary troponin at 0 and 3 hrs.
- 4 Trials with >1000 patients
- Identified approximately 25% as low risk
- 30 day MACE = 0.6%
*Addendum 08/15/2018: Received an email from Ben Mati, MD at Ventura County Medical Center was working on his grand rounds talk on low risk chest pain and added a few more studies to make this table more current. The Oliver et al study did not have the number of patients with HEART Score ≤3, but Ben emailed the lead author and found out the number was 255.
Is there anything more we can do to decrease this risk?
- Kind of hard to get to less than 0.8% risk, but this is where shared decision making comes in
- Hess et al published The Chest Pain Choice Trial in 2012 [6]
- 204 patients
- Usual Care vs Decision Aid
- Patients felt more informed with the decision aid
- I tell my patients at this point in your work up, for every 100 patients who come in to the ED with chest pain and negative results like yourself, 1 in 100 will have a heart attack or pre-heart attack diagnosis in the next 30 days. So we really have 3 options:
- Admit you to the observation unit for stress testing, however this could lead to a false positive test and more testing (It’s hard to get to less than 0.6%)
- Discharge you home to follow up with your primary care doctor in the next 30 days for further evaluation of your chest pain?
- If you don’t have a primary care doctor I can get you an appointment in one of our clinics in the next 30 days to further evaluate this chest pain.
- I then document whatever conversation and decision is made in the patient chart.
Clinical Bottom Line:
- Clinical Judgment = HEART Score 0 – 3 minus caveats discussed
- Relevant Scientific Evidence = External Validation of HEART Score 0 – 3 + Cardiac Troponin at 0 and 3 hours
- Patient Values and Preferences = Shared Decision Making
References:
- Than M et al. A 2-h diagnostic protocol to assess patients with chest pain symptoms in the Asia-Pacific region (ASPECT): a prospective observational validation study. Lancet 2011; 377 (9771): 1077-84. PMID: 21435709
- SJ Aldous et al. A new improved accelerated diagnostic protocol safely identifies low-risk patients with chest pain in the emergency department. Acad Emerg Med 2012; 19 (5): 510 – 6. PMID: 22594354
- Than M et al. 2-Hour accelerated diagnostic protocol to assess patients with chest pain symptoms using contemporary troponins as the only biomarker: the ADAPT trial. J Am Coll Cardiol 2012; 59(23): 2091 – 8. PMID: 22578923
- Sun B et al. Assessment of Chest Pain in the Emergency Department. Circulation 2015; 132: A13647. Abstract Only
- Backus BE et al. Risk Scores for Patients with Chest Pain: Evaluation in the Emergency Department. Curr Cardiol Reviews 2011; 7(1): 2 – 8. PMCID: PMC3131711
- Hess EP et al. The Chest Pain Choice Decision Aid: A Randomized Trial. Circ Cardiovasc Qual Outcomes 2012; 5(3): 251 – 9. PMID: 22496116
- Sun BC et al. Comparison of the HEART and TIMI Risk Scores for Suspected Acute Coronary Syndrome in the Emergency Department. Crit Pathw Cardiol 2016; 15 (1): 1 – 5. PMID: 26881812
For More On This Topic Checkout:
- Rob Orman on ERCast: Amal Mattu on Low Risk Chest Pain
- Rob Orman on ERCast: Which Chest Pain Patients can be Discharged?
- Low-Risk Chest Pain ADP Showdown (Using TIMI vs HEART): Part 1 of 3
- Low-Risk Chest Pain ADP Showdown: Part 3 of 3 – Delta Troponins and Stress Tests
Post Peer Reviewed By: Anand Swaminathan (Twitter: @EMSwami) and Barbra Backus (Twitter: @barbrabackus)
The post Management and Disposition of Low Risk Chest Pain appeared first on REBEL EM - Emergency Medicine Blog.