
 Case Presentation: A 4-year-old previously healthy Hispanic female presented to the ED with a diffuse rash and facial swelling, concerning for an apparent allergic reaction. She was rushed into the treatment area for evaluation of possible anaphylaxis and respiratory assessment. She was tachycardic with a heart rate in the 130s, tachypneic, and borderline hypotensive for her age. Initial exam was negative for wheezing or stridor, but she had edema to the face and neck with a red raised rash covering her face. Epinephrine, Benadryl, and Solumedrol were ordered STAT given concern for airway compromise secondary to a severe anaphylactic reaction.
Case Presentation: A 4-year-old previously healthy Hispanic female presented to the ED with a diffuse rash and facial swelling, concerning for an apparent allergic reaction. She was rushed into the treatment area for evaluation of possible anaphylaxis and respiratory assessment. She was tachycardic with a heart rate in the 130s, tachypneic, and borderline hypotensive for her age. Initial exam was negative for wheezing or stridor, but she had edema to the face and neck with a red raised rash covering her face. Epinephrine, Benadryl, and Solumedrol were ordered STAT given concern for airway compromise secondary to a severe anaphylactic reaction.
Additional information from mom revealed no prior history of anaphylaxis, no new food/medication ingestions or topical exposures, no known allergies, and no significant past medical history. Of note, she had been seen in the ED three days earlier, diagnosed with Strep Pharyngitis, and discharged after treatment with IM Penicillin G. The patient was tearful, ill appearing, and withdrawn. On a quick review of systems, mom reports that over the last five days she initially had a high fever (102o F) and sore throat, followed by anterior neck swelling on day 2, with vomiting, diarrhea, and the rash presenting on day 4. On secondary examination, she was noted to be febrile in the ED, and physical exam was significant for diffuse blanching maculopapular rash, tender cervical lymphadenopathy, dry lips, conjunctivitis, and bilateral hand and foot edema and erythema. While her presentation was most consistent with Kawasaki disease, given the current pandemic required Multisystem Inflammatory Syndrome in Children following COVID-19 exposure (MIS-C) was also high on the list of differential diagnoses. Other diagnoses considered included: other viral exanthems (EBV, CMV, measles, adenovirus), Scarlet Fever, Toxic Shock Syndrome, Staphylococcal Scalded Skin Syndrome, Stevens-Johnson Syndrome, allergic reaction, and sepsis.
ED Course:
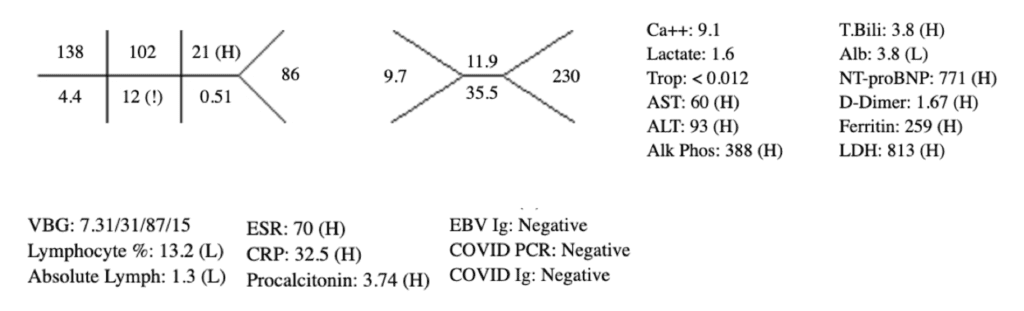
Considering MIS-C as a likely alternative diagnosis, a slower approach to fluid resuscitation was utilized instead of the traditional 20 cc/kg bolus used in sepsis/septic shock to better monitor her fluid status given the potential for fluid overload and the rapid development of acute heart failure. Initial resuscitation was started with a 10 cc/kg bolus of NS. Her vital signs and repeat physical exam were essentially unchanged following the first bolus, so an additional 10 cc/kg bolus was administered. Ceftriaxone and Vancomycin were also initiated in the ED with blood and urine cultures pending at the time of admission. EKG showed sinus tachycardia and Chest XR in ED was negative for pneumonia or any other acute cardiopulmonary findings. Additional laboratory workup is seen below. She was admitted to the Pediatric ICU for further management of Kawasaki Disease vs MIS-C.
Discussion:
Although this patient was negative for COVID antigens and antibodies, it is possible that she may have cleared the infection by the time she developed KD symptoms. Furthermore, it is important to note that the novelty of the virus leads to uncertainties regarding the sensitivity and specificity of COVID-19 RT-PCR testing and antibody detection and interpretation. Many recent studies, although limited by size and duration, have shown that these Kawasaki-like symptoms can develop weeks after exposure to COVID-19, and the majority of patients are not acutely infected with the virus at the time of presentation (5). On the one hand, antibodies are generally fairly reliable four weeks post infection, though there are some cases that have shown that even in patients with positive RT-PCR results, almost 19% may be IgG seronegative at four weeks following exposure and up to 40% after eight weeks (3).
There is also significant overlap in symptomatology and pathophysiology of the two disease processes. Initial studies have provided strong evidence showing that COVID preferentially targets the protein angiotensin-converting-enzyme 2 (ACE2) on endothelial cells resulting in a systemic vasculitis similar to that seen in KD (6). This evidence is further supported by the fact that MIS-C generally presents with physical exam findings consistent with a diagnosis of atypical KD. Additionally, in both severe MIS-C and KD Shock Syndrome, there may be associated left heart systolic dysfunction and significant hypotension requiring vasoactive medications for hemodynamic support (1). It is also known that KD has been associated with multiple viruses, including the seasonal coronavirus strain linked to the common cold. With this knowledge and understanding, it may be more appropriate to describe this disease process as COVID-19 associated KD instead of trying to differentiate between MIS-C and KD (2). It is very possible that MIS-C has been improperly classified as a separate entity from KD, when perhaps it is the same post-viral process, we have been studying for years with Kawasaki Disease, simply with the addition of a newly identified “Pathogen X.” The major difference in this case is that SARS-Cov-2 would be the first virus simultaneously linked to Kawasaki Disease and a global pandemic.
Considering these factors, in combination with the high prevalence of asymptomatic COVID carriers within the population, the presence of GI symptoms, and lab results that were consistent with an acute inflammatory syndrome, MIS-C remained high in the list of differential diagnoses.
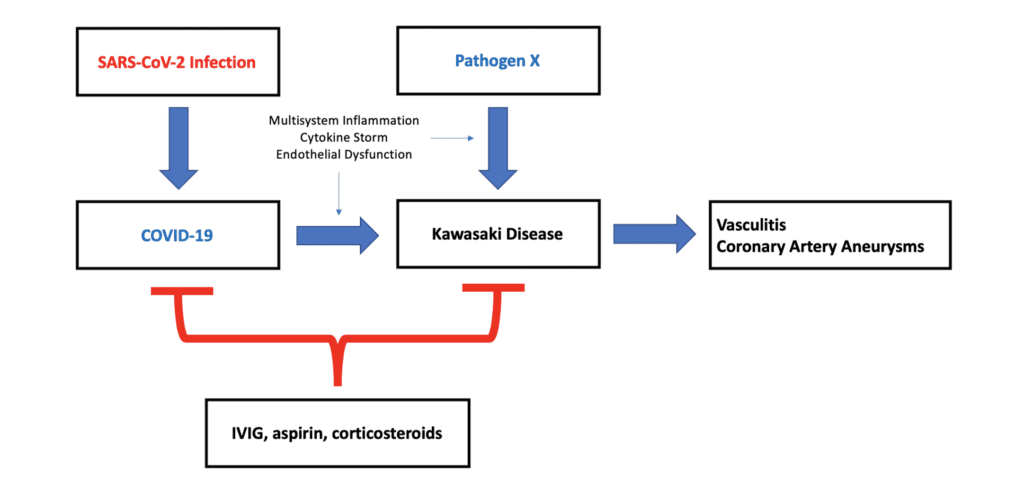
Figure 1. Possible Link Between COVID-19 and KD
Diagnosis:
There is no single test that provides a definitive diagnosis of KD. The diagnosis is based on clinical presentation and supported by characteristic laboratory abnormalities. According to the AHA, in order to make a diagnosis of Typical KD, a child must have a fever for at least five days AND have four of the five additional physical exam findings:
- Conjunctivitis (bilateral, painless, non-purulent)
- Mucocutaneous changes (cracked lips, strawberry tongue, erythema, pharyngitis)
- Polymorphous rash (diffuse, macular, may be scarlatiniform)
- Extremity changes (erythema, edema, desquamation)
- Lymphadenopathy (generally cervical and unilateral)
Patients with fewer than 4 of the above findings are considered to have Atypical KD.
Regarding the laboratory evaluation, almost all inflammatory markers and acute phase reactants are elevated given the disease’s association with acute inflammatory process. CRP > 3 and ESR > 40 are seen in both typical and atypical KD. More severe disease, termed Kawasaki Shock Syndrome, often requires the use of vasopressors for hemodynamic support and is associated with increasingly high levels of CRP, Procalcitonin, d-dimer, and IL-6 (8). Leukocytosis and thrombocytosis are also common findings. Hypoalbuminemia is associated with increased disease severity due to microvascular permeability and resultant peripheral edema. Elevations in NT-proBNP and troponin reflect cardiac inflammation and edema as opposed to myocardial ischemia (1). Other findings of undefined significance include lymphopenia, elevated LFTs, hyponatremia, hyperbilirubinemia, and sterile pyuria.
Future options for testing include the use of serum and urinary biomarkers that have been found to be directly elevated in response to KD and later improve with IVIG administration (7).
Case Conclusion:
She received treatment with IVIG upon admission and had an uncomplicated inpatient course. Transthoracic echocardiogram showed normal cardiac structure and function with no evidence of proximal coronary artery aneurysm or ectasia. Initial urinalysis was consistent with UTI but repeat urinalysis the day following admission was negative. Stool PCR studies were positive for Enteropathogenic E. coli (EPEC). She continued to improve and was transferred to the floor after two days in the Pediatric ICU. Blood and urine cultures were also negative after 48 hours and antibiotics were discontinued. Parotid gland ultrasound showed cervical LAD. She was discharged on hospital day #4 with a diagnosis of Kawasaki Disease based on her negative COVID studies and relatively quick recovery. Her parents were instructed to continue giving her aspirin daily for continued prevention of complications related to coronary artery aneurysm. She is scheduled to follow up with pediatric cardiology in two weeks for repeat echocardiogram.
Guest Post By

C. Blair Gaines, MD
Emergency Medicine, PGY-3
Jackson Memorial Hospital
Miami, FL
References:
- Belhadjer Z et al. Acute Heart Failure in Multisystem Inflammatory Syndrome in Children (MIS-C) in the Context of Global SARS-CoV-2 Pandemic. Circulation 2020. PMID: 32418446
- Calabri GB et al. COVID-19 and Kawasaki Disease: A Glimpse at the Past for a Predictable Future. Pediatric Cardiology 2020. PMID: 32462467
- Long QX et al. Clinical and Immunological Assessment of Asymptomatic SARS-CoV-2 Infections. Nature Medicine 2020. [Link is HERE]
- Ramphul K et al. Kawasaki Disease: A Comprehensive Review. Archives of Medical Science – Atherosclerotic Diseases 2018. PMID: 30775588
- Sandhaus H et al. Association Between COVID-19 and Kawasaki Disease: Vigilance Required From Otolaryngologists. Otolaryngology – Head and Neck Surgery 2020. PMID: 32423291
- Sardu C et al. Hypertension, Thrombosis, Kidney Failure, and Diabetes: Is COVID-19 an Endothelial Disease? A Comprehensive Evaluation of Clinical and Basic Evidence. Journal of Clinical Medicine 2020. PMID: 32403217
- Seaton K et al. Evidence-Based Management of Kawasaki Disease in the Emergency Department. Pediatric Emergency Medicine Practice 2015. [Link is HERE]
- Toubiani J et al. Kawasaki-Like Multisystem Inflammatory Syndrome in Children During the COVID-19 Pandemic in Paris, France: Prospective Observational Study. BMJ 2020. PMID: 32493739
- Xu S et al. COVID-19 and Kawasaki Disease in Children. Pharmacological Research 2020. PMID: 32464327
Post Peer Reviewed By: Mizuho Morrison, DO (Twitter: @mizuhomorrison) and Salim R. Rezaie, MD (Twitter: @srrezaie)
The post Multisystem Inflammatory Syndrome in Children (MIS-C) vs Kawasaki Disease appeared first on REBEL EM - Emergency Medicine Blog.