
 Background: Peri-operative anaphylaxis is an unexpected complication of intubation. The major life threat in anaphylaxis is typically loss of airway, however profound hypotension and circulatory collapse are still possible life threats even in the setting of a protected airway. Peri-operative anaphylaxis is considered an important enough issue to be the subject of the NAP 6 (National Audit Project) audit this year in Great Britain. (Reporting period November 2015 – November 2016).
Background: Peri-operative anaphylaxis is an unexpected complication of intubation. The major life threat in anaphylaxis is typically loss of airway, however profound hypotension and circulatory collapse are still possible life threats even in the setting of a protected airway. Peri-operative anaphylaxis is considered an important enough issue to be the subject of the NAP 6 (National Audit Project) audit this year in Great Britain. (Reporting period November 2015 – November 2016).
Anaphylaxis to ketamine and etomidate are extremely rare. There are only sporadic case reports of anaphylactoid reactions to each of these agents. Rocuronium and succinylcholine, on the other hand, are divalent molecules that make it easier for IgE mediated anaphylaxis to occur than with other agents such as vecuronium and atracurium, even in the setting of no previous exposure. Allergic reactions to neuromuscular blocking agents are almost exclusively IgE mediated. First time exposures account for 75% of patients having reactions.
Historical estimates of anaphylaxis have been flawed by difficulties defining the denominator of exposures, and by the challenges of catching and confirming a significant anaphylaxis event. Previous perioperative anaphylaxis rates have been as low as 1:10,000 – 1:20,000. A Japanese survey found rates of 1:18,000. (237 total cases, 13 cardiac arrests, one death). [Japanese Society of Anesthesiology data](password protected for JSA members, figures reported in [3]).
The denominator of exposures can be over estimated when it is based on drug usage figures taken from drug sales. This discounts wasted vials, expired vials, multiple vials used on a single patient, or vials opened and not used. Health systems that do not have robust perioperative anaphylaxis follow up procedures may not be able to confirm true anaphylaxis events, and may not catch every event that occurs. Mild anaphylaxis events may not be noticed, as they would occur in patients whose airways were already managed, who were covered by drapes that obscure any skin manifestations, and in patient who are unable to verbalize / describe their symptoms.
Do We Really Know the True Rates of Pre-Intubation Anaphylaxis? [1]
- A New Zealand study at two hospitals in Auckland sought to better define the true rates of perioperative anaphylaxis in their population.
- Retrospective, observational cohort study of intraoperative anaphylaxis to neuromuscular-blocking drugs (NMBDs) at two hospitals between 2006 and 2012.
- Most facilities used an electronic anesthetic medical record.
- All cases of suspected perioperative anaphylaxis were referred to the same allergy clinic.
- Anaphylaxis was confirmed based on a combination of:
- clinical description
- tryptase levels
- skin testing to all peri-anesthetic agents
- Along with an assessment of cross reactivity. Positive (histamine) and negative (saline) controls were used for skin testing.
- These were high grade anaphylaxis events, including profound hypotension, and intraoperative cardiac arrest.
-
Results:
- 92,858 anesthetic cases involving new exposures to NMB’s.
- 21 patients with anaphylaxis confirmed out of 89 patients referred to allergy clinic.
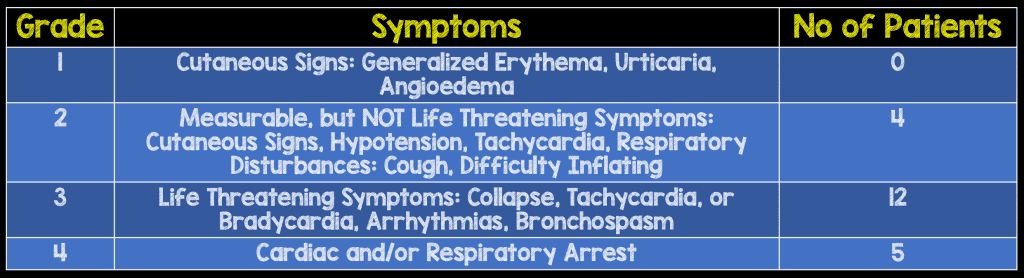
Adapted from Mertes, J Investig Allergol Clin Immunol 2011 [2]
- Despite the severity of some of the anaphylaxis events, (including a V-fib arrest) there were no deaths reported.
- With anaphylaxis events occurring in new exposures to both succinylcholine and rocuronium it has been suggested that IgE sensitization to these drugs could be triggered by exposures to other environmental and pharmacologic antigens.
-
Rates of confirmed anaphylaxis to neuromuscular blocking agent:
- Succinylcholine: 1:2,079
- Rocuronium: 1:2,498
- Atracurium: 1:22,450
-
Strengths:
- Closed population with single clinic follow up
- Extensive efforts made to establish anaphylaxis diagnosis
- Well described process of skin testing (positive and negative controls described)
-
Weaknesses:
- Single city, (2 hospitals).
- Possible genetic/geographic differences in the NZ population that make these numbers difficult to reproduce.
- Small number of total anaphylaxis events
- Authors Conclusion: “In Auckland, the rate of anaphylaxis to succinylcholine and rocuronium is approximately 10-fold higher than to atracurium. Previous estimates of NMBD anaphylaxis rates are potentially confounded by inaccurate proxies of new patient exposures. This is the first study to report anaphylaxis rates using a hard denominator of new patient exposures obtained direct from anesthetic records.”
Does Sugammadex Affect Anaphylaxis to Rocuronium? [3]
- Sugammadex had a delayed entry into the US market due to concerns over sugammadex-induced anaphylaxis (1:18,000).
- Due to its mechanism of action of encapsulation of the rocuronium molecule sugammadex has been suggested as a possible treatment agent for rocuronium induced anaphylaxis.
- Lab based studies show that the allergenic ammonium groups on rocuronium are still able to interact with IgE antibodies when encapsulated by sugammadex. Another study showed that basophil activation, once started, could not be blocked when sugammadex was added.
- There are several clinical case reports, and case series of patients that have improved after receiving sugammadex for rocuronium induced anaphylaxis.
- Reasons for this include the effect of concurrent anaphylaxis management (epinephrine, IV fluid), and that reversing paralysis could improve venous return and preload due to an increase in muscle tone in the lower extremities.
- There are no current expert recommendations to include sugammadex in anaphylaxis algorithms.
What Does Pholcodine Exposure Have to Do With Peri-Intubation Anaphylaxis? [4]
There are geographical differences in anesthetic anaphylaxis rates. These could be due to variations in exposures to sensitizing agents. One example is Pholcodine. This is an opioid cough suppressant that has been implicated in facilitating an increase in IgE mediated hypersensitivity reactions. Pholcodine was removed from the market in Sweden in the late 1980’s. Recent studies have found rates of anaphylaxis to neuromuscular blocking agents to be 10 times higher in Norway than in Sweden. Removing pholcodine from the market in Norway has lowered the incidence of NMB agent anaphylaxis. The counter argument to this theory is that IgE sensitization to pholcodine and morphine occurs in countries such as the USA and the Netherlands despite low pholcodine consumption. This suggests that other environmental exposures are responsible for IgE sensitization.
Where Should we Document NMB Anaphylaxis?
In a PulmCrit (EMCrit) Post by Josh Farkas on April 6th, 2016, the excellent suggestion that patients with known difficult airways have this documented as a rocuronium allergy. The notes section can then describe the issues pertinent to their airway management. It will be important to clarify whether the patient has a true allergy to rocuronium, or if they are ‘just’ a difficult intubation.
Cross Reactivity:
For those patients with anaphylaxis from rocuronium, the rates of cross reactivity on skin testing to other neuromuscular blocking agents are high: succinylcholine 44%, vecuronium 40% (45 patients). For those with anaphylaxis to Succinylcholine, cross-reactivity rates were lower, but still significant: rocuronium 24%, vecuronium 12% (17 patients). This data is from a Western Australia study evaluating neuromuscular blocking drug anaphylaxis with robust allergy clinic follow up [5]. Due to these high rates of cross-reactivity between NMB agents, Takazawa et al. [3] recommend a NMB free intubation for these patients.
Clinical Take Home Points:
- Be aware of anaphylaxis to NMB as a cause of post intubation hypotension.(1:2000-1:2500)
- Sugammadex is unlikely to reverse rocuronium induced anaphylaxis.
- If a patient has a neuromuscular blocking agent listed on their allergy list, this is a real entity, and cross reactivity to other agents can exist: proceed with caution, and consider a KSI (Ketamine Sequence Intubation) HT Reuben Strayer MD.
References:
- Reddy JI et al. Anaphylaxis Is More Common with Rocuronium and Succinylcholine than with Atracurium. Anesthesiology 2015; 122(1): 39 – 45. PMID: 25405395
- Mertes PM et al. Reducing the Risk of Anaphylaxis During Anesthesia: 2011 Updated Guidelines for Clinical Practice. J Investing Allergol Clin Immunol 2011; 21(6) 442 – 53. PMID: 21995177
- Takazawa T et al. Sugammadex and Rocuronium-Induced Anaphylaxis. J Anesth 2016; 30: 290 – 97. PMID: 26646837
- Florvaag E & Johansson SG. The Pholcodine Story. Immune Allergy Clin North Am 2009; 29(3): 419 – 27. PMID: 19563989
- Sadler PH et al. Anaphylaxis to Neuromuscular Blocking Drugs: Incidence and Cross-Reactivity in Western Australia from 2002 to 2011. Br J Anaesth 2013; 110(6):981 – 7. PMID: 23335568
Post Peer Reviewed By: Salim R. Rezaie (Twitter: @srrezaie)
The post Peri-Intubation Anaphylaxis appeared first on REBEL EM - Emergency Medicine Blog.