
 Welcome back to the April 2016 edition of REBELCast. For this episode I was lucky enough to get Scott Weingart on the show to talk to us about all things Apneic Oxygenation (ApOx). ApOx is a concept that has been around for some time in the operating room literature, but only recently been gaining acceptance in the ED, especially after the publication of this concept by Scott and Richard Levitan in the Annals of Emergency Medicine in 2011 [1]. Many nay sayers will argue that the OR studies were in controlled settings with elective surgical patients who were not in critical condition. The believers would argue that ApOx makes sense, its low cost, and low complexity. To date there has been no randomized controlled trials (RCTs) on ApOx in the ED. There has been one ICU Trial (i.e. The FELLOW Trial) [2] and an even more recent observational trial in the ED [3] that have been published on the topic of ApOx. So the question remains: Is Apneic Oxygenation Overhyped?
Welcome back to the April 2016 edition of REBELCast. For this episode I was lucky enough to get Scott Weingart on the show to talk to us about all things Apneic Oxygenation (ApOx). ApOx is a concept that has been around for some time in the operating room literature, but only recently been gaining acceptance in the ED, especially after the publication of this concept by Scott and Richard Levitan in the Annals of Emergency Medicine in 2011 [1]. Many nay sayers will argue that the OR studies were in controlled settings with elective surgical patients who were not in critical condition. The believers would argue that ApOx makes sense, its low cost, and low complexity. To date there has been no randomized controlled trials (RCTs) on ApOx in the ED. There has been one ICU Trial (i.e. The FELLOW Trial) [2] and an even more recent observational trial in the ED [3] that have been published on the topic of ApOx. So the question remains: Is Apneic Oxygenation Overhyped?
REBEL Cast Episode 25: Is Apneic Oxygenation Overhyped with Scott Weingart
Click here for Direct Download of Podcast

Associate Professor of Emergency Medicine
Chief of Division of Emergency Critical Care
Stony Brook School of Medicine, Stony Brook, NY
Twitter: @emcrit
Blog: emcrit.org
What are Preoxygenation (PreOx), Apneic Oxygenation (ApOx), and Reoxygenation (ReOx)?
Preoxygenation (PreOx)
- Should be broken up into 2 separate terms: Preoxygenation and Denitrogenation
- Denitrogenation = Washing out as much nitrogen from the lungs so that you have a buffer/bag of oxygen when the patient isn’t breathing
- Requires Time: 3 min of tidal volume breathing on a high FiO2 source
- With a Non-rebreather (NRB) mask alone, you are giving approximately 60% FiO2 which will make it impossible to accomplish denitrogenation
- Preoxygenation (PreOx) = Getting the O2 saturation as close to 100% before pushing RSI meds to intubate
Apneic Oxygenation (ApOx)
- This occurs during the time from pushing intubation medications, which is anywhere from 45 – 60 seconds, while the paralytic is taking effect, that the patient is burning through their oxygen stores
- Apneic Oxygenation (ApOx) = Passive movement of oxygen to the alveoli without the patient having to breath and without you having to breath for them
- Apneic CPAP = Little Brother of ApOx; In patients who have closed alveoli or flooded alveoli; Essentially used for maintenance of recruitment of alveoli during apneic period
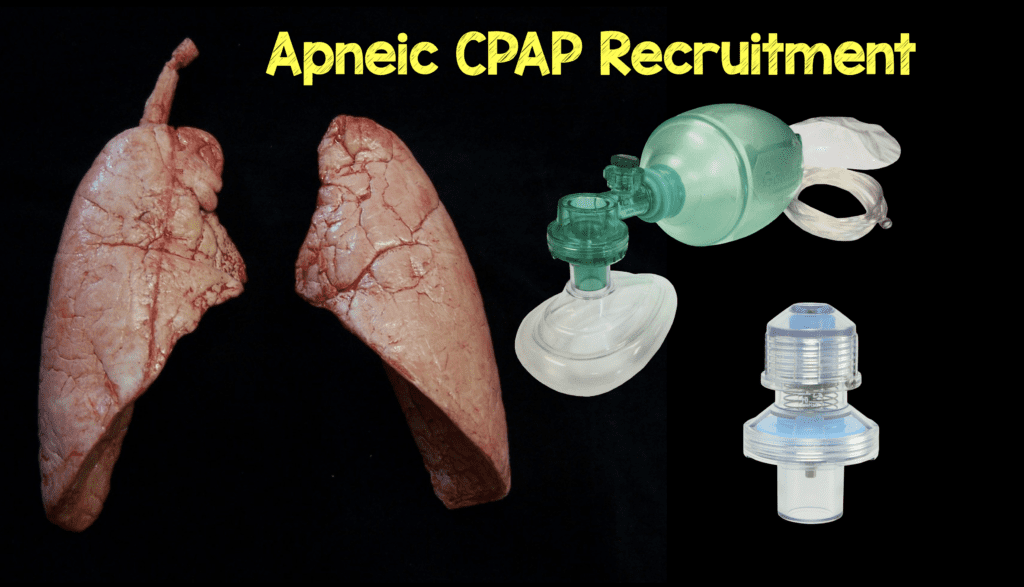
Apneic CPAP Recruitment = BVM + PEEP Valve + NC (Represents BEST PreOx, ApOx, & ReOx Currently Available)
Reoxygenation (ReOx)
- Reoxygenation (ReOx) = Attempts to increase O2 sats when a patient drops their sats during airway management
- If patient has physiologic shunt physiology, standard BVM will not suffice to fix patients desaturation in between attempts at intubation
BOTTOM LINE: PreOx, ApOx, and ReOx are all attempts to avoid the deadly DeOx (Deoxygenation)
What are your thoughts on the The Fellow Trial? [2]
-
Summary of Trial:
- Randomized Controlled Trial (RCT) of 150 Critically Ill Patients in a Single ICU
- Randomized to Apneic Oxygenation vs Usual Care
- Study Conclusion: Use of Apneic Oxygenation vs Usual Care Made no Difference in the Lowest Arterial Oxygen Saturation Between Induction and Two Minutes After Completion of Intubation
-
Issue with Usual Care in this Trial:
- Majority of patients had BVM during apneic period
- Most ED patients are not fasted and using BVM could potentially cause vomiting
- Not maintaining an open pathway from the nares to the glottis for patients not being bagged
- Combination of these 2 things hurt the take home message of the study
- Majority of patients had BVM during apneic period
Does Apneic Oxygenation help in patients with pulmonary shunt physiology (i.e. pulmonary edema, multifocal pneumonia, etc…)?
- ApOx will help if it is being given with Apneic CPAP
- Without CPAP, ApOx will not work in patients with shunt physiology
- Bagging with BVM alone will give O2 and PEEP but again we really want to avoid bagging our patients in the ED as this can cause vomiting
- With this strategy ApOx may be superfluous
- A better strategy might be NC at 15 LPM + BVM (without bagging) and with a PEEP Valve
- This will provide both O2 and CPAP without requiring bagging (Check Out this Amazing 2 Min Demonstration HERE)
What are your thoughts on the Observational ED Trial recently published by Sackles et al? [3]
-
Summary of Trial:
- Observational trial in a single ED of 635 patients who received either ApOx or No ApOx
- Study Conclusion: ApOx in Adult Patients Undergoing RSI had better 1st pass intubation without hypoxemia with a NNT of 7.6
-
The Fact that this Trial is Observational:
- For People Who Believe in ApOx: Helpful trial that confirms their belief structure
- For People Who Don’t Believe in ApOx: Does not change their minds, because this is still only observational data
- Bottom Line: We need an ED RCT on ApOx
Can you walk us through your exact approach to preoxygenation in a septic patient with pneumonia who is tachypneic, hypoxic, and hypotensive?
-
The Physiologically Difficult Airway (HOp Killers)
- Hypotension
- Oxygenation (i.e. Hypoxemia)
- pH and Ventilation
-
How to Manage our Patient with Hypotension and Hypoxemia
-
Oxygenation (i.e. Hypoxemia)
- Place patient on standard nasal cannula (NC) at 15L
- BVM with PEEP valve with 2 hand mask seal for 3 minutes (NO NEED TO BAG) for preoxygenation and denitrogenation
-
Hypotension
- RSI Meds (Great Explanation HERE)
- Ketamine IV 0.5 mg/kg
- Rocuronium IV 1.6 – 2.0 mg/kg
- Start norepinephrine drip or push aliquots of push-dose epinephrine
- Norepinephrine IV 0.01 – 1 mcg/kg/min
- Push-Dose Epinephrine IV 5 – 20 mcg every 2 – 5 min
- RSI Meds (Great Explanation HERE)
-
Oxygenation (i.e. Hypoxemia)
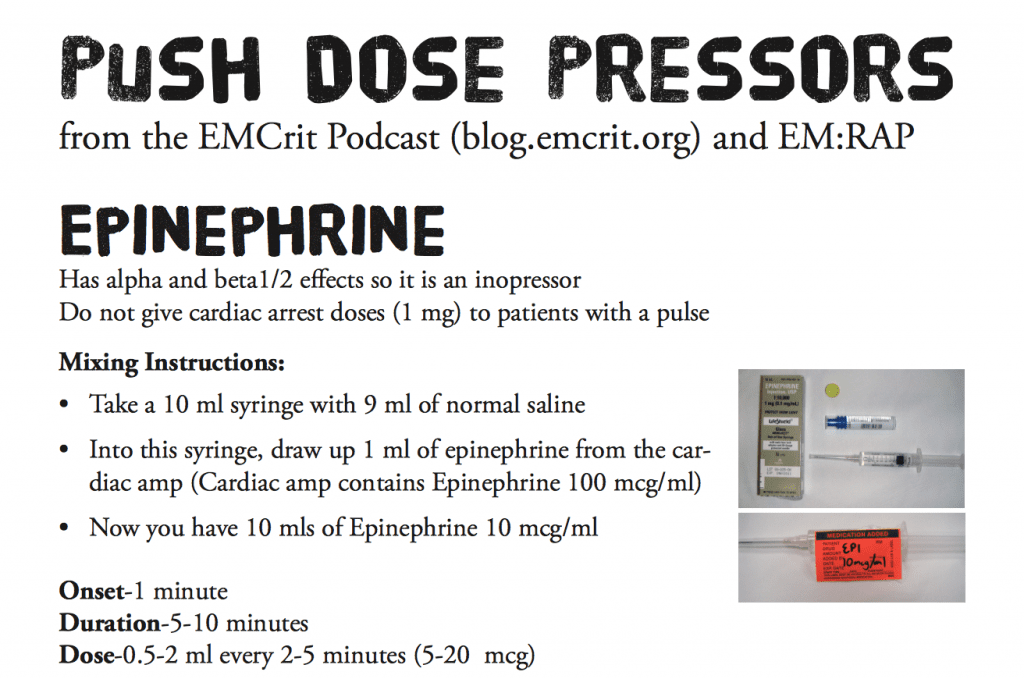
Image Borrowed from emcrit.org
Is there a patient we should not use ApOx in?
-
We know ApOx Works in Patients Without Shunt Physiology
- THRIVE Trial: Transnasal humidified Rapid-Insufflation Ventilatory Exchange [4]
- 25 patients with difficult airways undergoing general anesthesia
- Median Apnea was 14 minutes
- No patient experienced O2 Sat <90%
- THRIVE Trial: Transnasal humidified Rapid-Insufflation Ventilatory Exchange [4]
- Most Modalities we use for Pre-Oxygenation and Denitrogenation are NOT good enough on their own (i.e. Non-Rebreather Mask)
- BOTTOM LINE: There is no reason at this time to not be using nasal cannula for ApOx with intubation
Take Home Messages:
- PreOx is getting the O2 saturation as close to 100% before pushing RSI meds to intubate
- ApOx is passive movement of oxygen to the alveoli without the patient having to breath and without you having to breath for them
- In patients with pulmonary shunt physiology, a better strategy might be NC at 15LPM + BVM (Without Bagging) + a PEEP Valve because this will provide both O2 and CPAP for alveolar recruitment
- The Physiologically Difficult Airway = HOp Killers
- Hypotension
- Oxygenation (i.e. Hypoxemia)
- pH and Ventilation
- There is no reason at this time to not be using nasal cannula for ApOx with intubation
BONUS Question:
Lets say for a moment that you are not Scott Weingart. You are working as a faculty at a teaching institution and you have a resident approach you saying they had just listened to the EMCrit podcast. They want to try something because they heard it on the podcast. How would you handle that situation?
- Things discussed on the EMCrit podcast are things that are able to be done in the environment of an ED ICU with fellows, which is different than what most people have.
- In general, as a resident you shouldn’t say you heard something on a podcast and want to do it:
- Puts people in a tough situation
- Its important to read the primary literature behind what is being said
-
As the attending who is hearing this, a good way to handle this is telling the resident:
- Lets discuss this more after we get our patient stabilized
- Lets do a journal club on this and see if this is something we can incorporate into our practice
For More on This Topic Checkout:
- Scott Weingart on EMCrit: Podcast 158 – The FELLOW Trial on Apneic Oxygenation in ICU Patients
- Rory Spiegel on EMCrit: More on the FELLOW Trial
- Scott Weingart on EMCrit: Apneic CPAP Recruitment Demonstration by George Kovacs
- Salim Rezaie on REBEL EM: Preoxygenation and Apneic Oxygenation
- Salim Rezaie on REBEL EM: The FELLOW Trial: An End to Apneic Oxygenation?
- Salim Rezaie on REBEL EM: Should we be Using Apneic Oxygenation (ApOx) in the ED?
References:
- Weingart, Scott D, and Richard M Levitan. Preoxygenation and prevention of desaturation during emergency airway management. Ann Emerg Med 2011; 59 (3): 165 – 75. PMID: 22050948
- Semler MW et al. Randomized Trial of Apneic Oxygenation During Endotracheal Intubation of the Critically Ill. Am J Respir Crit Care Med 2015 [Epub ahead of print] PMID: 26426458
- Sackles JC et al. First Pass Success Without Hypoxemia is Increased with the Use of Apneic Oxygenation During RSI in the Emergency Department. Acad Emerg Med 2016. [epub ahead of print] PMID: 26836712
- Patel A et al. Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE): a physiological method of increasing apnoea time in patients with difficult airways. Anesthesia 2015; 70: 323 – 329. PMID: 25388828
Post Peer Reviewed By: Anand Swaminathan (Twitter: @EMSwami)
The post REBEL Cast Episode 25: Is Apneic Oxygenation Overhyped with Scott Weingart appeared first on REBEL EM - Emergency Medicine Blog.