
 Take Home Points on Tracheostomy Emergencies
Take Home Points on Tracheostomy Emergencies
- Track is mature in 7 days – don’t blindly replace before then because concern for false track creation
- All bleeding needs to be taken seriously and should be evaluated by surgery
- If not ventilating through trach – go through it systematically to find malfunction
REBEL Core Cast 12.0 – Tracheostomy Emergencies
 What is a trach?
What is a trach?
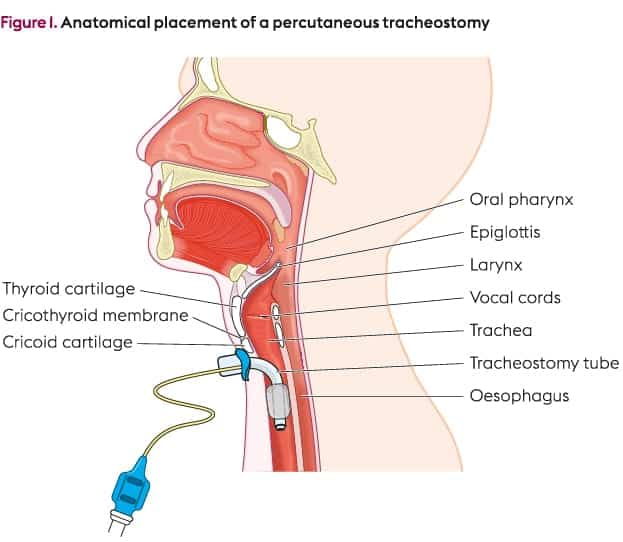
Permanent or semi permanent airway BELOW the glottis. It is most commonly placed between 3rd and 4th tracheal rings into the trachea.
Trachs are placed for 4 MAJOR reasons:
- Bypass glottic or supraglottic stenosis or obstruction
- Tracheal toilet
- Provide more comfortable airway for patients requiring prolonged ventilation
- Protect from aspiration
Management:
Key Concept: Takes 7-10 days for tract to become mature. If >7 days out, can replace trach safely.
Obstruction and Dislodgement are the commonly seen complications in the emergency department
-
Dislodgement
-
If trach greater than 7 days old you can simply replace it. Make sure you know patients current trach size.
-
To replace trach, follow these simple steps
- Take new trach and load obturator
- Apply some lubrication to the trach
- Take trach and enter the stoma at 90 degree angle
- As trach passes skin angle it down, straight down into trach
- Once in place, pull obturator and place inner cannula
-
To replace trach, follow these simple steps
-
If trach less than 7 days old do not replace because you could create false track.
- Use fiberoptic scope
- Get ENT or Surg involved to help with placement
- If trouble replacing trach you can bag through the stoma. Use LMA or Pediatric mask with BVM to supply oxygen.
- Bagging not working? Can’t replace the stoma? You gotta intubate from above.
-
If trach greater than 7 days old you can simply replace it. Make sure you know patients current trach size.
-
Obstruction
-
Address patient hypoxia -> supplemental O2 via mouth with 100% non-rebreather or assisted breaths with BVM
- Need to deflate cuff in order to get oxygen through
- Attempt to pass suction catheter. If unable to pass suction cath then trach or inner canula needs to be replaced.
-
Address patient hypoxia -> supplemental O2 via mouth with 100% non-rebreather or assisted breaths with BVM
Replacement trach:
- Sometimes difficult to replace trach with same sized one, its ok to downsize.
- You can replace with ETT, would recommend using 6.0 cuffed tube.
Bleeding Trach:
- Mild bleeding at skin – likely local irritation. Treat with pressure and possibly silver nitrate
- Bleeding from trach should be taken seriously, need to consider the life threatening tracheo-innominate fistula.
- Due to trach eroding anteriorly causing abnormal connection between the trachea and the innominate or right subclavian artery.
- Consult CT surgery, likely will need bronchoscopy
-
Temporizing measures while waiting for definitive treatment
- Over-inflate the cuff to tamponade bleeding
- Secure airway with endotracheal intubation
- Remove tracheostomy and insert a finger to compress innominate artery anteriorly
For More on This Topic Checkout:
- LITFL: Tracheostomy
- Crashing Patient: Traceostomy and Trach Emergencies
- Core EM: Tracheostomy Issues
- emDocs: Trach Travails
- emDocs : Management of Acute Respiratory Distress in a Tracheostomy Patient
Shownotes Written By: Miguel Reyes, MD (Twitter: @miguel_reyesMD)
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post REBEL Core Cast 12.0 – Tracheostomy Emergencies appeared first on REBEL EM - Emergency Medicine Blog.