¿EXISTE LA POSIBILIDAD DE QUE SEA EL UNICO, O DE LOS POCOS QUE SE HAN LEIDO Y Han ENTENDIDO ESTO DE LOS UNIFORMES EN SITUACIONES DE RIESGO "TACTICAS"?
NO SOLO ES PARECER, TAMBIEN DEBEMOS SER...
DONT SHOOT THE EMS "PARAMEDIC"
#DONTSHOOTEMS #DONTSOOTPARAMEDIC #Tacticool #ChamanTacticoMD

Pueden analizar esta foto con los fines de ver un sinergismo de potencializacion de recursos y competencias, casa incendiada, amenaza real en su interior para bomberos y rescatistas, pues un escudo de seguridad y proteccion armada para evitar mayor dao por el incendio, al mismo tiempo evitar poner en peligro real a los bomberos y demas respondedores. #DrRamonReyesMD Excelente ejemplo de una situacion Tactica tipo TECC Tactical Emergency Casulty Care. Un tirador activo en la ciudad de Boston, EUA. Incendia su casa el riesgo de que se afectaran mas viviendas por el incendio y por ende mayor riesgo de victimas, Se inicia sofocacion del fuego por los Bomberos de la Ciudad con proteccion con escudos balisticos y custodiados por el Equipo SWAT de la ciudad... Gracias Christian Goring, NREMT-P Boston EUA. por el aporte de la foto. https://emssolutionsint.blogspot.com/2018/03/tactical-medics-vs-rescue-task-force.html #StopTheBleed #BleedingControl #Tourniquet #Torniquete #PHTLS #ACLS #TACMED #MEDIVAC #TACEVAC #CASEVAC #CoTECC #CoTCCC #TECC #TCCC #MilitaryMedicine #Spain #HartfordConsensus #ATLS #Trauma #EMS #RemoteMedicine #TECCSpain #Intraosseous

Cuando busques un curso, piensa en el precio, avales, recursos de simulación en el curso, recursos didácticos, perfil de los instructores, credibilidad de los instructores, certificaciones de los instructores, en esto no es válido quien tenga mejor diseñador gráfico, nombre más TACTICOOL, fotos más chuliguay... Cuantos trapos se tira encima el instructor, sellitos, parches, equipos de airsoft, entre otras parafernalias. Si es por fotos... ufff Investiga, ¿Quien es ese RAMBO? ¿Es reconocido por instituciones reconocidas? ¿Se vale de sellos como Stop The Bleed, El Rojo de TECC, ASOCIACIONES MEGA MUNDIALES, que solo existen en un logo muy chuliguay? Pues esos son datos que te llevan a la duda. La gran mayoría de esos, no les he visto en reunión de facultados de TCCC en la NAEMT, no les he visto en la reunión del Comité C-TECC, no son reconocidos como instructores por instituciones como la NAEMT, la AHA, etc. Entonces. ¿Que son? Para mi falsos profetas. by Dr. Ramon Reyes, MD

CURSO TACTICAL CASUALTY CARE FOR LAW ENFORCEMENT & FIRST RESPONDER

Updated
Graham Medical on Oct 8, 2019 10:00:00 AM
Everyday Emergency Medical Services (EMS) responders provide an important service in treating and transporting patients with minor injuries up to serious, life-threatening conditions. While highly trained and skilled, neither the Emergency Medical Technician (EMT), nor the Paramedic was ever meant to be an expert in mass casualty incidents such as an active shooter event. Just as police units have regular patrol and also SWAT, medical responders also need specialized response teams.
Specialized Teams Provide Faster Patient Care
Enter the tactical medic and rescue task force concepts. Both tactical medics and rescue task force personnel provide emergency care at the scenes of heavy casualty incidents where scenes are not always secure. Tactical medics and task force personnel work very closely with law enforcement in emergency situations. Yet, there are distinct differences in the type of care and response protocol provided as described in this EMS1.com article.
Rescue task forces are primarily created by a quick assembling of responding EMS personnel, paramedics, and fire personnel. Tactical medics are often specifically attached to a response team like SWAT.
Rescue Task Forces
In past active shooter incidents, there have been communication lags and delays in care when responding. During these delays, precious life-saving minutes tick away for the injured victims.
A rescue task force is, in short, a coordinated response that allows access to victims faster.
Rescue task forces prioritize stabilization, extrication and transport for further care for patients. This is the opposite of care models that prioritize triage first.
Without a designated rescue task force, the different participating organizations must figure who should take the lead and when it is safe to provide care. Rescue task forces designate a lead for these situations, and divide responses based on hot, warm, and cold zones of the incident. By responding from a centralized staging zone, EMS can quickly deploy to cleared areas and provide point of wound care.
Rescue task forces generally consist of specially trained EMS responders that are on their regularly scheduled shift.
Tactical Medics
Usually called in for emergency responses, medics show up in full uniform of the unit to which they are attached, such as a SWAT team. The tactical medic will provide initial medical care as needed to victims, bystanders and perpetrators once the scene is secured, but they may be there, primarily, to provide medical aid to the team members.
The tactical medic will generally transfer patient care to a standard EMS unit if further care and transportation to the hospital are needed.
Another way that you can distinguish these two teams is that rescue task force members wear a standard daily uniform (i.e. fire or police) and are typically dispatched during their normal shift. Their uniforms may be supplemented with tactical vests as needed for safety. Tactical medics wear the uniform of the tactical team they are attached to, often including body armor. Tactical medics are physically located within the team, or may stay just outside of the hot zone.
Graham Medical is proud to be able to provide EMS products to help first responders do their job more effectively and efficiently.
Graham Medical works to make patient transport faster, easier and safer to promote better outcomes in an emergency. For more information on EMS products, contact us here or visit Grahammedical.com.

 #TactiCool Ficcion vs Realidad by #ChamaTacticoMD
#TactiCool Ficcion vs Realidad by #ChamaTacticoMD


#TactiCool Ficcion vs Realidad by #ChamaTacticoMD


#TactiCool by #ChamanTacticoMD
Active Shooter Incidents: The Rescue Task Force Concept
by ROBERT MUECK Wed, September 20, 2017
The concept of the Rescue Task Force (RTF) came from the Arlington County (Virginia) Fire Department. Looking at active shooter events around the country, these fire department leaders created a model that enables emergency medical services (EMS) to provide emergency medical intervention faster and within the Incident Command System (ICS) construct.
Robert Mueck headshotKnown as “warm zone integration,” the RTF concept uses the phrase “Task Force,” which is an ICS term for a unit consisting of mixed resources assembled to meet a specific tactical need. Regardless of the name, the RTF should be able to integrate easily into public safety agencies anywhere. The RTF consists of EMS and law enforcement personnel who work together to provide immediate basic medical care to victims. This differs from Tactical EMS, which usually focuses on medical care for the responders.
The Current EMS System
Civilian EMS personnel are not combat medics, so they do not go into the line of fire like their counterparts may in the military. In a traditional response to an incident involving gun violence, EMS personnel set up in a staging area and await word from law enforcement that the building is declared clear and secure. However, when people are bleeding out and dying in mass casualty incidents, the urgency of medical care is being pushed to new limits.
As part of the RTF concept, three zones must be understood:
The Hot Zone – The area where there is a known hazard or threat to life that is potentially direct and immediate. This includes any uncontrolled area where the active shooter could directly engage people.
The Warm Zone – The areas where law enforcement has either cleared or isolated the threat, and the risk is minimal or has been mitigated. This area may be considered clear but not secure.
The Cold Zone – The area where there is little or no threat. It may include the outside of the building or an area law enforcement has secured. It is safe to operate in this zone.
In its initial stages, an active shooter incident in a building makes the entire building the hot zone. Law enforcement personnel immediately move toward the shooter to stop the attack and prevent more injuries or deaths. As law enforcement personnel move inside and begin to secure parts of the building, these areas become warm zones because there is some certainty that the shooter is not in the immediate vicinity. This is where EMS personnel could have an opportunity to join law enforcement and make entry to locate and treat victims, even as other officers search for and neutralize the suspect. Keep in mind that incidents with multiple shooters make this more difficult for first responders.
What the RTF Concept Offers
The RTF concept focuses on the needs and care of victims, not responders. EMS members of the RTF work with patrol officers to deliver immediate medical intervention for readily treatable injuries, like severe bleeding and airway compromise. The team then stabilizes victims for evacuation to definitive care.
The RTF provides “point of wound” care to victims where there is an ongoing threat. These teams (there may be more than one) treat, stabilize, and remove the injured in a speedy fashion under the protection of armed law enforcement. Although the RTFs operate in the warm zone, they do not engage in triage. Injured persons encountered by RTF teams are treated as they are reached. People who can walk without assistance are directed to self-evacuate down a cleared corridor under law enforcement direction (within the warm zones).
This process requires coordination between law enforcement and EMS personnel. Incident command needs to direct the RTF to locations where they are needed. That means the RTF would probably be under law enforcement command, but the RTF is essentially a unified command asset.
Initially, those first on the scene – both bystanders and victims – may provide aide to one another before responders arrive. First responders may direct them to provide aide to each other until the RTF reaches them. Injured victims may eventually be placed in a casualty collection point (CCP) before being moved to a cold zone, where they can be transported to definitive care. Where survivors are placed is determined by initial responders and should be communicated to the RTF teams through unified command.
Challenges for Implementation of This Model
The RTF model presents some challenges. Members should be equipped with the proper tools – including Kevlar helmets and body armor – to operate in dangerous environments. This may prove to be an issue for EMS, as EMS organizations often include volunteers. Issues of purchasing the equipment, sizing protective gear to fit EMS staff, and storing additional tools and equipment in ambulances can prove difficult.
As local jurisdictions adopt the RTF concept, it is important everyone involved understand how teams will operate. There is no “one way” to develop an RTF. The important issue is that law enforcement and EMS know how to integrate and understand their own written policies to work as an RTF. Policies and training dictate how they interface during a response. Although there may be some differences from one area to the next, the basics remain the same: identify those wounded, determine the need for emergency medical care, and extract those injured to a CCP. Patients eventually are evacuated to an external CCP well outside the building to a secure location where traditional EMS care is initiated.
As with any emergency incident, it is important to achieve mutual communications to coordinate the RTF during an incident. This requires training together and conducting drills so the coordination of the RTF becomes second nature. Failing to train together can reveal challenges that were not considered in the planning phase. For example, RTF officers provide security for EMS personnel as they move into the building and down corridors secured by initial contact teams. These escort officers cannot wander off once they get EMS on site. They need to understand their role and remain in place to provide security for the medics while they treat victims.
When public safety staff members are unarmed, it is known upfront that these members would not be part of the initial entry. However, if members are trained to assist in rendering emergency first aid, they can be proactive and perform a critical task. EMS resources may be limited, so having personnel assist could go a long way in saving lives. However, the RTF concept only works if personnel have what they need to participate.
Providing Additional Medical Assistance
If staff cannot participate in an RTF, they could still render assistance to responders. They may assist in establishing an internal CCP near a secure entry point, where casualties can be grouped to allow for faster and more efficient evacuation by non-RTF EMS personnel. Having body movers available for staff may allow them to assist in moving victims from a warm zone to a cold zone. Having them trained and equipped in the use of tourniquets and hemostatic gauze, for example, may make staff invaluable for saving lives.
Beyond traditional first responders, it is important to remember the first “first responders,” which are the people on the scene when the incident happens. For example, stocking up on bleeding control kits and training staff in using tourniquets as part of the “Stop the Bleed” campaign may save lives. For all facilities or institutions, though, understanding the RTF is critical to understanding what to do to save lives. Being an armed or unarmed agency does not prevent personnel from rendering aid. The training and background of these agencies may make their staff good candidates for the RTF.
Robert Mueck is an adjunct associate professor of public safety administration and homeland security at University of Maryland, University College; and director of public safety at St. John’s College in Annapolis, Maryland. He currently serves as: an active member of the Governors Workgroup on Active Assailant Response in Maryland; an adjunct faculty member for the Texas A&M Engineering Extension Service (TEEX); and a sector chair for the Maryland Chapter of Infragard. He formerly was the training coordinator at the George Washington University in Washington, D.C., for the University Police and the Consortium of Universities of the Washington Metropolitan Area. He retired after a 29-year career at the University of Maryland Police Department (UMPD), having served in a variety of capacities in operations, administration, and command positions. https://www.domesticpreparedness.com/healthcare/active-shooter-incidents-the-rescue-task-force-concept/
TCC-LEFR
TECC
TCCC Tactical Combat Casualty Care Handbook
TACMED España
BCon Saber un poco mas sobre control de sangrados
Hartford
Tactical Medics vs Rescue Task Force
GUIA DE SOPORTE VITAL PARA SEGURIDAD PRIVADA COMO PRIMER INTERVINIENTE EN INCIDENTES ARMADOS. by Juan Jose Pajuelo Castro y David Grevillen Carretero. SEMES 2018
http://emssolutionsint.blogspot.com.es/2018/02/guia-de-soporte-vital-para-seguridad.html

Mochilas a prueba de balas nueva tendencia en inicio escuela en los EUA emssolutionsint.blogspot.com/2018/09/mochilas-prueba-de-balas-nueva.html


PROTOCOLO PARA INTERVENCIONES DE SOPORTE VITAL EN INCIDENTES DE MÚLTIPLES VÍCTIMAS POR ATENTADOS TERRORISTAS ABRIL 2016 (Actualizado Marzo 2018) by Juan Jose Pajuelo
http://emssolutionsint.blogspot.com.es/2018/03/protocolo-para-intervenciones-de.html
8 trampas a evitar en el controlhemorragias
Guia de Soporte en Incidentes con Amenaza para Primer Interviniente Policial by Juan Jose Pajuelo Castro
emssolutionsint.blogspot.com/2018/07/guia-de-soporte-en-incidentes-con.html
emssolutionsint.blogspot.com/2018/07/guia-de-soporte-en-incidentes-con.html
TACTICAL COMBAT CASUALTY CARE Handbook version 5 May 2017
emssolutionsint.blogspot.com/2017/07/tactical-combat-casualty-care-handbook.html
emssolutionsint.blogspot.com/2017/07/tactical-combat-casualty-care-handbook.html
Updated TCCC Guidelines (31 JAN 2017) "Actualizacion 2017 de las Guias" Tactical Combat Casualty Care
emssolutionsint.blogspot.com/2012/07/presentacion-del-programa-phtls-tccc.html
emssolutionsint.blogspot.com/2012/07/presentacion-del-programa-phtls-tccc.html
TCCC TACTICAL COMBAT CASUALTY CARE Quick Reference Guide First Edition 2017 FREE PDF
emssolutionsint.blogspot.com/2018/07/tccc-tactical-combat-casualty-care.html
emssolutionsint.blogspot.com/2018/07/tccc-tactical-combat-casualty-care.html
Updated TCCC Guidelines (31 JAN 2017) "Actualizacion 2017 de las Guias" Tactical Combat Casualty Care emssolutionsint.blogspot.com.es/2012/07/presentacion-del-programa-phtls-tccc.html
MANUAL DE SOPORTE VITAL AVANZADO EN COMBATE Ministerio de Defensa España 2014
ttp://emssolutionsint.blogspot.com.es/2016/02/manual-de-soporte-vital-avanzado-en.html
COMTOMS TACTICAL MEDIC HANDBOOK 2013 Edition
emssolutionsint.blogspot.com/2016/12/guias-para-el-manejo-de-heridos-en.html
emssolutionsint.blogspot.com/2018/07/manejo-de-heridos-en-incidentes.html
TERRORISMO Y SALUD PÚBLICA - "GESTIÓN SANITARIA DE ATENTADOS TERRORISTAS POR BOMBA"
emssolutionsint.blogspot.com/2013/08/terrorismo-y-salud-publica-gestion.html
TRAUMA DE TORAX: DOCENA DE LA MUERTE en trauma toracico
https://emssolutionsint.blogspot.com.es/2013/01/penetrating-chest-trauma-photo-trauma.html
75th Ranger Regiment Trauma Management Team (Tactical) Ranger Medic Handbook FREE pdf
emssolutionsint.blogspot.com.es/2018/02/75th-ranger-regiment-trauma-management.html
SPECIAL OPERATIONS FORCES Medical Handbook Free PDF
emssolutionsint.blogspot.com/2018/02/special-operations-forces-medical.html
emssolutionsint.blogspot.com/2018/02/special-operations-forces-medical.html
Balística de las heridas: introducción para los profesionales de la salud, del derecho, de las ciencias forenses, de las fuerzas armadas y de las fuerzas encargadas de hacer cumplir la ley
http://emssolutionsint.blogspot.com/2017/04/balistica-de-las-heridas-introduccion.html
http://emssolutionsint.blogspo
Guía para el manejo médico-quirúrgico de heridos en situación de conflicto armado by CICR
http://emssolutionsint.blogspot.com/2017/09/guia-para-el-manejo-medico-quirurgico.html
http://emssolutionsint.blogspo
CIRUGÍA DE GUERRA TRABAJAR CON RECURSOS LIMITADOS EN CONFLICTOS ARMADOS Y OTRAS SITUACIONES DE VIOLENCIA VOLUMEN 1 C. Giannou M. Baldan CICR
http://emssolutionsint.blogspot.com.es/2013/01/cirugia-de-guerra-trabajar-con-recursos.html
http://emssolutionsint.blogspo
Manual Suturas, Ligaduras, Nudos y Drenajes. Hospital Donostia, Pais Vasco. España http://emssolutionsint.blogspot.com/2017/09/manual-suturas-ligaduras-nudos-y.html
Manual CIERRE DE HERIDAS by ETHICON http://emssolutionsint.blogspot.com/2017/09/manual-cierre-de-heridas-by-ethicon.html
Manual de suturas. Menarini
http://emssolutionsint.blogspot.com/2017/09/manual-de-suturas-menarini.html
http://emssolutionsint.blogspo
Técnicas de Suturas para Enfermería ASEPEYO y 7 tipos de suturas que tienen que conocer estudiantes de medicina
http://emssolutionsint.blogspot.com/2015/01/tecnicas-de-suturas-para-enfermeria.html
http://emssolutionsint.blogspo
Cuaderno Enfermero.Cirugia Menor Heridas Suturas
http://emssolutionsint.blogspot.com/2016/07/cuaderno-enfermerocirugia-menor-heridas.html
http://emssolutionsint.blogspo
Manual Práctico de Cirugía Menor. Grupo de Cirugia Menor y Dermatologia. Societat Valenciana de Medicina Familiar i Comunitaria
http://emssolutionsint.blogspot.com/2013/09/manual-practico-de-cirugia-menor.html
http://emssolutionsint.blogspo
Protocolo de Atencion para Cirugia. Ministerio de Salud Publica Rep. Dominicana. Marzo 2016
http://emssolutionsint.blogspot.com/2016/09/protocolo-de-atencion-para-cirugia.html
http://emssolutionsint.blogspo
Manual de esterilización para centros de salud. Organización Panamericana de la Salud
http://emssolutionsint.blogspot.com/2016/07/manual-de-esterilizacion-para-centros.html
http://emssolutionsint.blogspo
Asistencia de salud en peligro: la importancia de proteger al personal de salud en zonas de guerra PDF Gratis
http://emssolutionsint.blogspot.com/2018/06/asistencia-de-salud-en-peligro-la.html
SERVICIOS PREHOSPITALARIOS Y DE AMBULANCIAS EN SITUACIONES DE RIESGO. PDF GRATIS
http://emssolutionsint.blogspot.com/2018/06/servicios-prehospitalarios-y-de.html
PDF Update on Prehospital Trauma Courses, NAEMT, Alex Eastman, Lieutenant and Deputy Medical Director, City of Dallas
http://emssolutionsint.blogspot.com.es/2016/12/phtls-prehospital-trauma-life-support.html
http://
SERVICIOS PREHOSPITALARIOS Y DE AMBULANCIAS EN SITUACIONES DE RIESGO. PDF GRATIS
http://
PDF Update on Prehospital Trauma Courses, NAEMT, Alex Eastman, Lieutenant and Deputy Medical Director, City of Dallas
http://
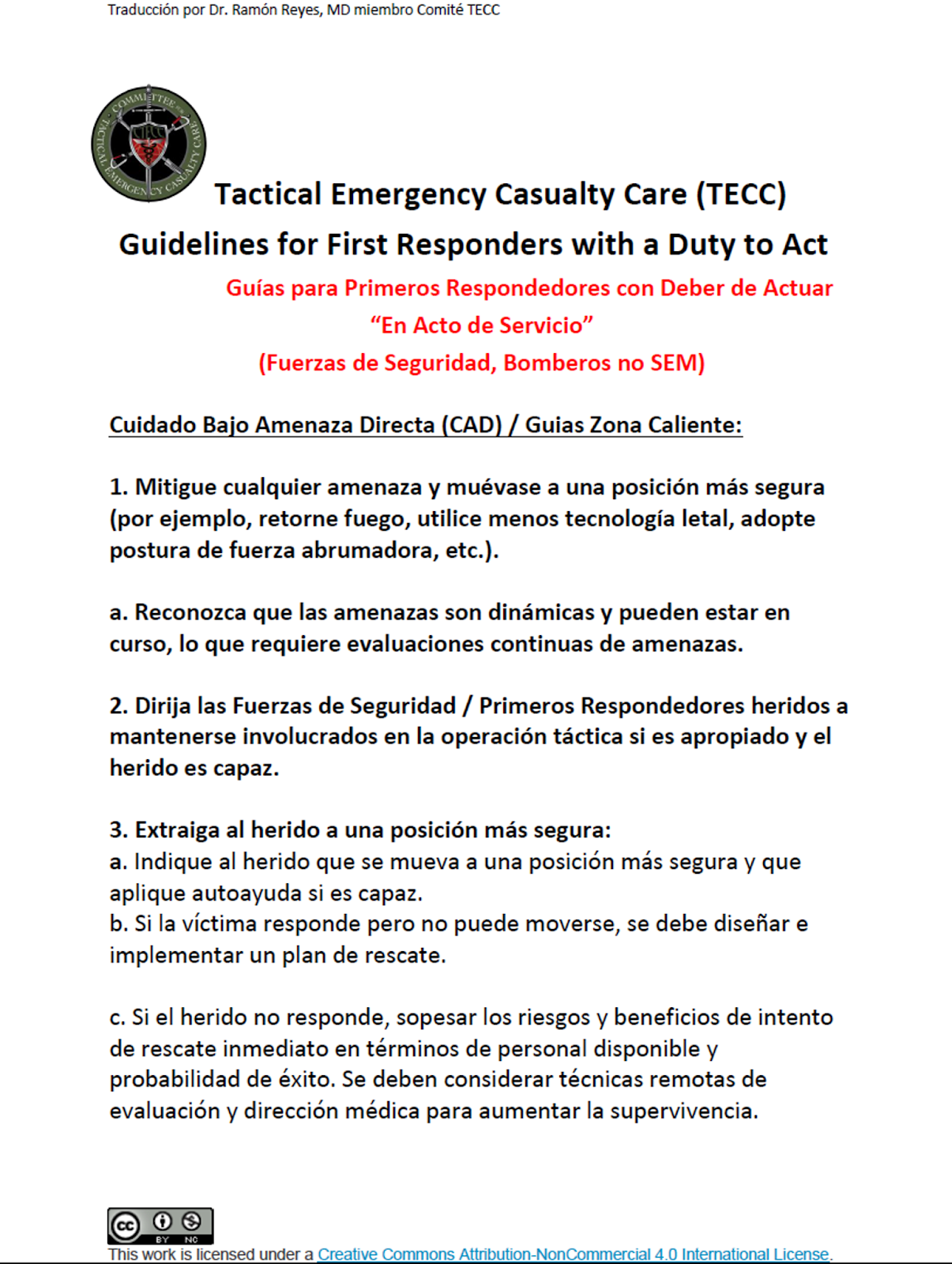
Tactical Emergency Casualty Care (TECC) Guidelines for First Responders with a Duty to Act Guías para Primeros Respondedores con Deber de Actuar “En Acto de Servicio” (Fuerzas de Seguridad, Bomberos no SEM) emssolutionsint.blogspot.com/2018/07/tactical-emergency-casualty-care-tecc.html
PAGINA FCEBOOK
MEDICINA TACTICA
Medicina
Del lat. medicīna.
Táctico, ca
Del lat. mod. tacticus, y este del gr. τακτικός taktikós, der. de τάσσειν tássein 'poner en orden'; la forma f., del lat. mod. tactica, y este del gr. τακτική taktikḗ.
1. adj. Perteneciente o relativo a la táctica.
2. adj. Experto en táctica. U. t. c. s.
3. f. Arte que enseña a poner en orden las cosas.
4. f. Método o sistema para ejecutar o conseguir algo.
5. f. Habilidad o tacto para aplicar una táctica.
6. f. Mil. Arte de disponer, mover y emplear la fuerza bélica para el combate.
Fuente http://www.rae.es #ChamanTacticoMD
Del lat. mod. tacticus, y este del gr. τακτικός taktikós, der. de τάσσειν tássein 'poner en orden'; la forma f., del lat. mod. tactica, y este del gr. τακτική taktikḗ.
1. adj. Perteneciente o relativo a la táctica.
2. adj. Experto en táctica. U. t. c. s.
3. f. Arte que enseña a poner en orden las cosas.
4. f. Método o sistema para ejecutar o conseguir algo.
5. f. Habilidad o tacto para aplicar una táctica.
6. f. Mil. Arte de disponer, mover y emplear la fuerza bélica para el combate.
Fuente http://www.rae.es #ChamanTacticoMD
 |
| Conjunto de Habilidades del C-TECC Segun el Nivel del Asistente |
Version 1
Version 2
Guías para Primeros Respondedores con Deber de Actuar “En Acto de Servicio”
(Fuerzas de Seguridad, Bomberos no SEM)
Enlace para descargar PDF Gratis
http://emssolutionsint.blogspot.com/2017/09/curso-tecc-espana-28-septiembre-2017.html

¿Es correcto que el SEM en situaciones Tacticas utilice uniformidad similar a la policial? Respuestas en video mañaña sabado 19 de mayo 2018. by Dr. Ramon Reyes, MD, EMT-Tactical, DMO
en nuestra pagina en facebook @drramonreyesmd https://www.facebook.com/DrRamonReyesMD/
Mas detalles en el enlace http://emssolutionsint.blogspot.com.es/2018/03/tactical-medics-vs-rescue-task-force.html
Rescue Task Force RTF? / FUERZAS de TAREA de RESCATE
 |
|
Guatemala military/medic special ops team. Art by Dansun Photos @DansunPhotos
Todos Nuestros VIDEOS en YouTube https://www.youtube.com/c/RamonReyes2015
Grupo en TELEGRAM Sociedad Iberoamericana de Emergencias
https://t.me/joinchat/FpTSAEHYjNLkNbq9204IzA
NO SOLO ES PARECER, TAMBIEN DEBEMOS SER...
El Dr. James Vretis, D.O es un MEDICO TACTICO, no parece, lo es... y lleva lo mismo que cualquier miembro de las Fuerzas del Orden...Porque el es Fuerza del Orden... ¿Es correcto que el SEM en situaciones Tacticas utilice uniformidad similar a la policial? Respuestas by Dr. Ramon Reyes, MD, EMT-Tactical, DMO en nuestra pagina en facebook @drramonreyesmd http://emssolutionsint.blogspot.com.es/2018/03/tactical-medics-vs-rescue-task-force.html
Dr. Ramon Reyes, MD https://www.facebook.com/DrRamonReyesMD/

Publicado en TWITTER
Que los ORCAS de Cataluña, son los unicos sanitarios a entrar a zona CALIENTE (Vamos que entrarn en CUF Zona de Fuego, Zona ROJA)... ¿Quien ha sido el experto de la NASA que se ha inventado esta cosa, que pondria en peligro inminente a Sanitarios DESARMADOS? Comentario by Dr. Ramon Reyes, MD
Cito Documento Original de TWITTER:
Els equips UIS (ORCAS) de @semgencat son els únics en accedir a zona “calenta” una vegada autoritzats per FFSS #simulacreTiradorActiu #emergenciesCOIB @COIBarcelona
http://emssolutionsint.blogspot.com.es/2018/03/tactical-medics-vs-rescue-task-force.html
Dejo compilacion de razones logicas y procedimientos Internacionales al respecto... Ni el TCCC, Ni TCC-LEFR, Ni CONTOMS, Ni CTECC, Ni nadie con algo de sentido comun diria o haria tal locura... Menos en España, pais de competencias muy claras y definidas, pais de islas profesionales... veremos el final de la peli.... como queda.

CONFUNDIR TACTICAL MEDICS VS. RESCUE TASK FORCE MEDICS, Pues tengo la ligera impresion es lo que han hecho en España, uniformar al personal sanitario, violando principios basicos de seguridad, al dejar bajo confusion total a quienes intervienen en la escena (Escena desde el principio especial y atipica), diferencia entre los RTF y EMS-T,
DEPAS-MADRID: El Dispositivo Especial Preventivo Actos Antisociales es un equipo constituido por 113 voluntarios que actúan en caso de manifestaciones, desalojos, altercados públicos o partidos de fútbol catalogados de alto riesgo.
ORCAS-CATALUÑA: Intervención sanitaria en atentados terroristas.
¿Es correcto que el SEM en situaciones Tacticas utilice uniformidad similar a la policial? Respuestas en video mañaña sabado 19 de mayo 2018. by Dr. Ramon Reyes, MD, EMT-Tactical, DMO en nuestra pagina en facebook Dr. Ramon Reyes, MD

RESPUESTA:
Mas detalles en el enlace
http://emssolutionsint.blogspot.com.es/2018/03/tactical-medics-vs-rescue-task-force.html
Rescue Task Force RTF? / FUERZAS de TAREA de RESCATE
En el dia de mañana trataremos este tema a fondo, para dejar claro, que ha sucedido en esta confusion, que podria realmente poner en peligro al personal sanitario.
Dr. Ramon Reyes, MD, EMT-T, DMO
Tactical Medical Specialist
TCCC-TECC Faculty
TCC-LEFR Medical Director
VP-Militar Comite Iberoamericano de Medicina Tactica y Operacional
Graduado de Tactical Protective Medical Support y Grupo de Entrenamiento Contra-Terrorismo del Gobierno de Estados Unidos
"NO SOLO ES PARECER, TAMBIEN DEBES DE SER" by Dr. Ramon REYES, MD
|
 Guatemala military/medic special ops team.Guatemala military/medic special ops team.Guatemala military/medic special ops team. Art by Dansun Photos @DansunPhotos
Guatemala military/medic special ops team.Guatemala military/medic special ops team.Guatemala military/medic special ops team. Art by Dansun Photos @DansunPhotos

Guatemala military/medic special ops team. Guatemala military/medic special ops team. Art by Dansun Photos @DansunPhotos

TACMED, Tactical Medicine, Active Shooting, Terrorism Attack.
Rescue Task Force is a new concept to SFD that is designed to get lifesaving medical treatment to victims in mass shootings quicker. The current standard fire/EMS response to the active shooter is to stage in a secure location until police mitigate the threat and secure the area to create a scene safe for fire/EMS operations. Unfortunately, while waiting for a secure scene, those injured inside the building aren't receiving care and are dying from their injuries. The RTF concept involves placing Paramedics in a forward position during an active shooter. The Paramedics are protected with cover and Police Officers, but are able to begin life-saving care much sooner than traditional
FUERZAS de TAREA de RESCATE "Rescue Task Force" RTF. es un nuevo concepto de los Servicios de Emergencias, ha sido diseñado para brindar tratamiento médico para evitar muertes prevenibles en víctimas durante tiroteos masivos y de manera más rápida y efectiva. La respuesta estándar actual ante fuego / SEM ante tiradores activos consiste en ubicarse en lugar seguro hasta que la policía suprima la amenaza y asegure el área para crear una escena segura para las operaciones de Bomberos / SEM. Desafortunadamente, mientras se espera una escena segura, los heridos dentro del edificio no estarán recibiendo atención y estarán muriendo por sus lesiones. El concepto de RTF implica colocar a los paramédicos en una posición en el frente durante un tirotesos activos. Los paramédicos estarán protegidos por cobertura (Escudos) y resguardos en la escena, ademas oficiales de policía,asi podran comenzar a salvar vidas mucho más rápido que con los métodos tradicionales de despliegue.
deployment methods.
TACTICAL MEDICS VS. RESCUE TASK FORCE MEDICS
What are the similarities and differences between these critical functions?
Written by
Jim Morrissey- ALCO EMS
Terrorism Preparedness Director
Senior SF FBI Tactical Medic
The simple answer is that tactical medics are “attached” to a tactical law enforcement team and are considered part of the team. Whereas a Rescue Task Force is a trained, but hastily formed group of EMS medical providers (private and/or fire based) that partner with law enforcement on scene and enter a newly secured area such as an active shooter incident, to provide triage, emergent care and extrication to the casualties.
 EMS uniforms: Does color matter? A majority of readers are most concerned about the color of their uniforms in regard to setting them apart from police officersFeb 16, 2017
EMS uniforms: Does color matter? A majority of readers are most concerned about the color of their uniforms in regard to setting them apart from police officersFeb 16, 2017







By EMS1 Staff
Gone are the days of all EMS providers wearing white pants, white shirt or a dark navy outfit.
And because of this variety, EMS1 columnist Catherine Counts looked at the impact and role uniform color plays. Specifically, she looked at research regarding police-public interactions and if EMS could benefit and change anything with the findings.
Uniforms are part of the first impression the community will have on the responding crew. (Photo/Hennepin EMS)
Uniforms are part of the first impression the community will have on the responding crew. (Photo/Hennepin EMS)
We asked our Facebook fans what color they thought paramedics should wear. A majority of commenters were most concerned about the color of their uniforms in regard to setting them apart from police officers. Others talked about the need for more high-visible clothing in EMS and their color preference based off weather resistance and job-related messes.
Do you think color matters? Let us know in the comments below.
1. "No badge. I'm a big fan of high visible uniforms, because this way at 3 a.m. we don't look like cops. I worked at one place where they had jumpsuits. As long as we don't look like cops. When we do, it tends to cause problems." — Brian Conner
2. "We have white tops and navy pants with BLS in all navy. I like how my uniform looks brand new. However, a white shirt is not practical for EMS providers day-to-day. Everything from fluids, to sweat stains, dirty footprints on your chest and even food. Without fail, I always spill my coffee the morning I wear a brand new shirt." — Denise Chagnon Beady
3. "I'm from Germany, and here it is a law that EMS providers have to wear high-visible clothes. So we have orange trousers, orange jackets and white shirts." — Moritz Werthschulte
4. "I agree to not having badges. I used to work for a private service and our class A's were 100 percent red. To me, that just screams 'medical' and I have yet to come across any LE that wears red. That's how it should be." — Luke Ailiff
5. "I've been mistaken for a police officer all of the time. I prefer the blues. I think they look professional. I have worn white shirt and blue pants and by the first 10 minutes they're already dirty. I prefer a blue polo shirt with EMS and professional licensure on back." — Brian Schilling
6. "Red shirts, black pants. Red and black are great at hiding stains, helps you to stay looking professional. Red doesn't retain much heat when working an MVC in the blistering Texas sun. Red is more flashy and EMS-related than blues, blacks and other dark colors and sets us apart from police officers, helps reduce danger as well. When I see gray, I think correctional officer. When I see beige, I think security guard." — Ari Andalman
7. "I would love a universal color coding. I also think we need to ditch the dark blue. I'm patriotic, but Europe is right to put their first responders that are not police into high visibility yellows and greens. I say fire should move toward a high visible yellow and red, and EMS should be high VI's yellow and royal blue." — Lawson C Stuart
8. "Ours are white. Not real practical, but the argument is that they want us to not look anything like our local LEOs who have blue and tan." — Adrian Hoesli
9. "Red. Easily recognizable and no confusion with law enforcement." — Jake Walker
10. "I like the idea of scrubs. Not just any type, though. Something specially designed for EMS in whatever colors a specific company is." — Britni Martinez https://www.ems1.com/ems-products/uniforms/articles/194890048-EMS-uniforms-Does-color-matter/
Class B Uniforms make us look like Cops
Mistaken Identity
Article Aug 31, 2008
This issue's close call was sent in by a reader who had a brush with violence and was almost drawn into the fray because of the badge on his uniform.
"My partner and I were at our usual convenience store/gas station at about 10:30 p.m. It's in a somewhat seedy neighborhood and was crowded. While we were in line, someone came running in and yelled, "They're fighting with guns outside!" As everyone else in the store ran toward the front windows to watch (why, I have no idea), we quietly sauntered to the back of the store. We got as far away as we could and called it in. We were stuck.
"Someone from outside came into the store again, looked at us and pleaded for us to help. 'Look at those police officers,' she added, gesturing toward us for the benefit of others in the store. 'They don't even care!' I calmly replied that we were paramedics, not police officers, and that the police would arrive soon. It didn't seem to register, and soon several people in the store were asking us why we weren't helping. The police arrived quickly, and two bad guys were arrested. My supervisor showed up, and as we were talking to him, someone approached us. 'Did you get the guy who did it?' he asked."
Over the years, EMS has grown serious roots in the arena of public safety. This identity has spawned similarities in the authority-based uniforms we often wear, which can resemble those worn by our public safety brethren. In this case, it almost put two EMSers in the middle of a dangerous situation.
Tactically, I applaud the medics for not getting involved in the fight. It may seem like a no-brainer when people are fighting with guns, but it took maturity and solid decision-making to stay back when urged to get involved by citizens.
This situation also provides a backdrop for bringing up some other safety and survival points:
Don't leave your ambulance running outside a store, even just for a minute. The ambulance here could have become a getaway vehicle for one of the shooters.
Remember the concepts of cover and concealment. If you ever find yourself in a situation such as this, look for something that will hide your body and protect you from bullets—this is cover. Examples include trees, brick walls and the engine block of your ambulance. Concealment is good in a pinch because it hides you, but it doesn't offer protection.
Retreat is always a strategy. Get away from the danger. Put as much space between you and any threats as possible. Go as far as you need to be safe—and then go a little further—until police secure the scene. Integrate cover and concealment while you are retreating.
Work through different situations in your head during down time. If you go to a store in a tough part of town (sometimes these are the only choices we have), come up with some safety strategies in the event things go bad (e.g., what if someone tried to jack your rig or steal your narcs?).
Carry a portable radio at all times. In this case, the medics had a link directly to the dispatcher. Most of us carry cell phones as well.
Communicate with your partner. The safety and survival strategies of a team may be greater than the sum of its individual efforts. Two heads are better than one.
Finally, don't forget the value of observation as a tactic. It's always better to observe a dangerous situation and avoid it than to have to use tactics to get out of it. Look for suspicious activity, drug or alcohol use and crowds gathering. Sometimes you can watch an area become "charged" or energized with activity prior to a violent outburst.
Other times an unusual silence is as valuable a sign of danger as suspicious activity.
Here is what the medics in this close call were wearing:
"Our uniforms have light-blue button-down shirts with a badge over the left chest and a nameplate on the right. There are patches on either shoulder also shaped like badges, along with patches to symbolize rank and years of service on the sleeves. Our uniforms are almost identical to those of several area police agencies, and nothing on them clearly identifies us as EMS workers."
What does your uniform look like, and why? While many like the authoritative-looking public safety uniform, others have moved to different styles (e.g., embroidered or screened polos) for a variety of reasons that include lower cost, comfort, practicality and (of course) safety.
Don't forget, a professional in a polo outperforms and looks better than a guy with a badge any day. It's the way you walk the walk.
Be careful out there.
To submit a case for review, e-mail Nancy.Perry@cygnusb2b.com.
Daniel D. Limmer, AS, EMT-P, is a paramedic with Kennebunk Fire-Rescue in Kennebunk, ME. He is the author of several EMS textbooks and a nationally recognized lecturer.
EMS EXPO™
Dan Limmer is a featured speaker at EMS EXPO, October 15–17, in Las Vegas, NV. For more information, visit www.emsexpo2008.com. https://www.emsworld.com/article/10320853/mistaken-identity






Both Tactical Medics and Rescue Task Force personnel provide emergent care in less than ideal situations, often under significant stress and in chaotic, sometimes hostile environments. Both work very closely with law enforcement during planning, training and actual events. Most Rescue Task Force members are outfitted with ballistic vests and helmets, and likewise, almost without exception, Tactical Medics are protected with body armor and helmets. Both Rescue Task Force and Tactical Medics are specifically trained and equipped to deal with ballistic, blast and other violence-induced trauma. Rescue Task Force members wear their usual daily uniform (Fire/ EMS/ law enforcement) and are typically dispatched during their normal shift. Tactical Medics wear the uniform of the tactical team they are attached to and are physically located with the team, or just outside of the “hot zone”.
Tactical Medics
Tactical Medics are somewhat analogous to the hockey team trainer who travels with the team and is there primary to provide medical aid to the team, whether the injury or ailment is serious or not. The most common items requested of the Tactical Medic are Band-Aids and ibuprofen. However, the Tactical Medic must also be prepared to provide life-saving interventions to team members and other on scene law enforcement. The Tactical Medic will provide initial medical care as needed to victims, bystanders, and perpetrators once the scene is secured. They will transfer patient care to a standard EMS unit if further care and transportation to the hospital is needed.
Tactical EMS models
Some law enforcement agencies (LEA) send officers/agents/deputies to EMT school, or comprehensive tactical medical classes and those officers may become the default Tactical Medic for the team. That may be a workable solution; however, it is unlikely those individuals have the medical experience and patient assessment skills needed to be the best medical practitioner in high-risk, high-stress situations.
There are countless workable models for the incorporation of a medical contingency plan for law enforcement operations. Some of the more common models are listed below:
- Officer/Agent/Trooper/medic- These are sworn law enforcement officers (LEO) having dual roles as an "operator" and medic; they have law enforcement powers and can certainly protect themselves from potential threats.
- Agency contract- In this case the LEA has a contract or MOU with a local EMS provider (Fire or private EMS service, or hospital medical group) to provide up-close medical care. Some agencies put the medics through a Reserve Officer school, so that they can be armed as LEOs.
- Individual contract- An individual or a team of individuals are under contract or MOU with the LEA for providing medical coverage for SWAT missions and training.
- ALS Stand by- In this outdated model, there are no Tactical Medics, but LE will stage a standard ambulance some distance away and they would respond to the scene after being secured by law enforcement.
There have been two major shifts in doctrine related to law enforcement operations over the last 10 years. One change focuses on aggressively going after active shooters with whatever assets happen to be on hand, instead of waiting for a SWAT team.
The second major change is recognizing the need for emergency medical contingency planning. This includes training all tactical personnel and line officers in the basics of self-care and buddy care with the focus on bleeding control and the addition of a dedicated Tactical Medic.
An aspect of this doctrine shift (in addition to the Tactical Medic) is - at minimum notifying –but ideally involving local EMS and hospitals about planned or developing law enforcement operations that have a high risk for injuries. SWAT teams are increasingly including a dedicated tactical medical component, and medical threat assessment as part of their organizational structure.
Learning about Tactical EMS
Many in the EMS/medical field have demonstrated and voiced interest in exploring what is required to get into the field of tactical medicine. In addition to the pre-existing medical training one already has (i.e. physician, nurse, paramedic, EMT, etc.), it is highly recommended to procure specific tactical medical education.
Programs such as NAEMT Tactical Combat Casualty Care (TCCC), Tactical Life Saver and others like it are one or two days in length and have been well received by the EMS and LE community. The International School of Tactical Medicine (ISTM) offers a 2 week intensive program aimed at medical practitioners who need basic training on law enforcement operations, and how to work within a law enforcement team as the medic.
Scenario of a tactical mission
On a typical planned SWAT operation there are several phases and steps that take place well before the “hit”. Most often, the mission is a planned high risk search or arrest warrant. After getting a "warning order", the SWAT team operators and all of the support elements (medical, communications, negotiators, etc.) typically convene at a Forward Staging Area (FSA).
A briefing will occur, where mission goals, subjects, and target location layouts are reviewed. Depending on the nature of the mission and Operations Security (OP-SEC) issues, the tactical medic may coordinate with the local EMS transport provider to have an ALS ambulance stage close to the location.
The Tactical Medic is the logical liaison to the on-scene EMS assets that support law enforcement operations. Typically the Tactical Medic will have a face-to-face meeting with EMS supporting units if they are available.
Rescue Task Force
Prompt integration of EMS medical rescue teams with Law Enforcement escort (Rescue Task Force) into an active shooter and other violent threat incidents is a recently adopted concept in the civilian first responder world. The introduction of the Rescue Tack Force (RTF) to the wounded casualties should be just after the threat has been eliminated, when the scene has been deemed relatively secure. Historically, Fire and EMS crews staged a distance away until LE methodically secured the scene before permitting EMS to access victims. This practice is being phased out and is being replaced with a more patient centric and life-saving approach.
There are two priorities in these types of events.
Eliminate the threat (LE responsibility)
Provide immediate life-saving interventions ASAP (everyone’s responsibility)
In terms of providing life-saving interventions, there are four ways to render medical aid in these types of situations.
Bystanders/ victims provide care to one another prior to any responder arrival.
LE rapidly extricates, escorts victims to a safe area where EMS is waiting and provides medical aid.
LE secures the area and THEY provide life-saving interventions at the point of wounding (POW).
LE secures the area and brings in the RTF under a force protection model.
The RTF focus should be on quick initial medical assessments and to provide life-saving interventions on scene at the point of wounding (POW) if needed. This should be done in concert with efforts to extricate victims to a Casualty Collection Point (CCP) where a secondary triage, treatment and transport can be provided. The RTF group should use a pre-entry LE/EMS checklist to insure important issues are addressed. The law enforcement aspect of the RTF is focused on escorting and protecting the medical member of the RTF. Urban Shield has been conducting several tactical and EMS/medical integrated scenarios each year since 2008. These scenarios are created to be realistic, tactically and medically challenging and create an obvious nexus between the tactical resolution and providing life-saving care to the casualties in a timely manner. The Urban Shield EMS Branch has a well-deserved reputation for creating some of the highest rated scenarios in Urban Shield. We aim to continue that trend.
The Rescue Task Force concept is becoming more widespread and adopted nationwide. Fire Departments, local EMS providers and law enforcement need to collaboratively train, drill and develop procedures and protocols for this concept to be effective. You do not want to be exchanging business cards the day of the horrific event.
PDF https://www.summahealth.org/~/media/files/summahealth/ems/ems-protocols/tactical-ems/tems%20protocol%20final.pdf

Tactical EMS: An overview
Learn about the basics of this rapidly evolving EMS subspecialty
Jul 31, 2013
What is a "SWAT medic" and what does it take to become one? Tactical medicine is a specialized and highly discriminating endeavor that requires intensive training, discipline and a unique relationship with law enforcement. Tactical medics have the primary responsibility of providing medical care to the SWAT team, but their duties extend far beyond that task.
This article examines the evolution, and current tactical medical principles and procedures employed by military and law enforcement agencies (LEA), specifically SWAT teams.
History
Tactical medicine concepts have been around since the dawn of medicine….and warfare. Even in early battles the “King’s Doctor” was to be close at hand to deal with injuries, but only to the royal few. Outcomes were not very good as the initial insult might have killed the victim; if that didn’t, then infection usually did.
Historical accounts and personal diaries of military medics through the centuries are fascinating and show a steady progression of tools and techniques and an ever improving understanding of injury management. The Vietnam War showed that rapid transport to a higher echelon of care had a significant impact on survival.
The last 10 years of conflict overseas has shown that controlling extremity hemorrhage and aggressive airway management accounted for a significant reduction in the casualty fatality rate (CFR). The CFR is the percentage of those who are wounded in battle die.1
Casualty Fatality Rate:
WWII 19.1 %
Vietnam War 15.8
Iraq/ Afghanistan conflicts 9.4
Prior to 2004, there were a significant proportion of deaths in American soldiers during the Global War of Terror (GWOT) associated with each of the following injuries:
Hemorrhage from extremity wounds
Junctional hemorrhage (where an arm or leg joins the torso, such as in the groin area after a high traumatic amputation)
Non-compressible hemorrhage (such as a gunshot wound to the abdomen)
Tension pneumothorax
Airway problems
It was noted that extremity hemorrhage was the most frequent cause of preventable battlefield deaths. The U.S. military re-introduced and emphasized tourniquet use and hemostatic agents with measurable success.
Tourniquets were proven to save lives on the battlefield including 31 lives saved in 6 months by tourniquets after the retraining. Kragh et al. estimated that 2000 lives were saved with tourniquets during the Iraq conflict. As importantly, there were no arms or legs lost because of tourniquet use.2
Causes of preventable battlefield death are not that different from the potential injuries of law enforcement/ SWAT operators during high-risk law enforcement operations.
Today's tactical EMS
Tactical medicine has become a discipline and specialty within law enforcement circles. High profile events such as the Columbine, Virginia Tech, Aurora Movie Theater and countless other “active shooter” incidents have shifted the way law enforcement operates.
There have been two major shifts in doctrine related to SWAT and law enforcement operations over the last 10 years. One change was focused on aggressively going after active shooters with whatever assets happen to be on hand, instead of waiting for a SWAT team.
The second has been to recognize the need for emergency medical contingency planning. This includes training officers/agents in the basics of “self-care” and “buddy care” with the focus on bleeding control.
Another aspect of this doctrine shift is the inclusion of organic assets (the tactical medic), and involving, or at least notifying local EMS, hospitals about law enforcement operations that have a high risk for injuries. SWAT teams have increasingly a dedicated tactical medical component as part of their setup.
Some law enforcement agencies (LEA) have decided to send officers to EMT school, or specific tactical medical classes. That may be a workable solution; however, it is unlikely those individuals have the experience and patient assessment skill needed to be the best medical practitioner they can be.
It may make more sense to train an experienced medic to work in a warm zone environment and keep the scope of that person's job as the medic.
Tactical EMS models
There are countless workable models for the incorporation of a medical contingency plan for law enforcement operations. Some of the more common models are listed below:
Officer-Agent/medic- sworn LEO having either dual roles as an "operator" and medic, or strictly as a medic; but has law enforcement powers and can certainly protect themselves from potential threats.
Agency contract: LEA has a contract or memorandum of understanding (MOU) with a local EMS provider to provide "up-close" medical care. Some agencies put the medics through a Reserve Officer school, so that they can be armed as LEOs.
Individual contract: An individual or a team made up of individuals who have either a contract or MOU between them and the LEA providing coverage for SWAT missions and training.
ALS Standby: No Tactical Medics, but ALS unit will stage close by and respond if scene is secured by law enforcement.
Learning about Tactical EMS
There are many in the EMS field that would like to explore the option of getting into the field of tactical medicine. In addition to the medical training one already has such as a physician, nurse, paramedic or EMT, it is highly recommended to procure specific tactical medical education.
Programs such as NAEMT Tactical Combat Casualty Care (TCCC) and other like it are one to two days in length and have been well received by the EMS community. The International School of Tactical Medicine (ISTM) offers a 2 week intensive program aimed at medical practitioners who need basic training on law enforcement operations, and how to work within a law enforcement team as the medic.
The emphasis in this program is to insure that the tactical situation is resolved and EMS providers are not put in harm’s way. There are many skills sessions and tactical/ medical scenarios to test the knowledge learned under stressful conditions.
The tactical medic
The Tactical Medic is the logical liaison to the on-scene EMS assets that support law enforcement operations. Typically the Tactical Medic will have a face-to-face meeting with EMS supporting units if they are available.
It is imperative that EMS providers are not put in harm’s way and are not allowed to enter a scene where there is a shooter, or other threats are still possible. In an active shooter type situation, once the threat is eliminated, the scene is no longer a hot zone. A quick sweep from a SWAT team can confirm this assumption.
If there are significant casualties, the next priority should be to escort the EMS providers into the scene quickly and safely into the newly created “warm zone." They would work closely with the Tactical Medic throughout the event.
Scenario of a tactical mission
On a typical hypothetical SWAT operation there are several phases and steps that take place well before the “hit”. Most often, the mission is a planned high risk search or arrest warrant. After getting a "warning order", the SWAT team operators and all of the support elements (medical, communications, negotiators, etc.) typically convene at a Forward Staging Area (FSA).
A briefing will occur, where mission goals, subjects, and target location layouts are reviewed. The tactical medic then calls the local EMS transport provider to have an ALS ambulance stage close to the location.
Most times if EMS is notified beforehand, they are welcome into the briefing. The local EMS crews are given instructions and a communications plan. In most cases they follow the vehicle convoy in and are in close proximity to the target location.
Local hospitals and trauma centers are notified that the mission is taking place and to be on alert in the event of casualties.
Personally, I’ve been on close to 200 SWAT missions and thankfully there have been no gun-fights with injuries.
On most of SWAT missions, we have a day or two to plan. Most large city police departments have a higher percentage of spontaneous SWAT missions such as a bank robbery “gone bad” or a barricaded subject.
Summary
Tactical medicine is an exciting and evolving field of emergency medicine. Consider taking a tactical medicine class and see if you are up to the task.
References
NAEMT Tactical Combat Casualty Care (TCCC) Curriculum, http://www.naemt.org/education/TCCC/tccc.aspx
Kragh J et al. Practical use of Emergency Tourniquets to stop Bleeding in Major Limb Trauma Journal of Trauma, 2008:64; 30-50 http://www.smcaf.org/InPressKragh.pdf
About the author
Jim Morrissey is a Tactical Paramedic for the San Francisco FBI SWAT team and the founder of the Tactical Medical Association of California (TMAC). Jim is also the Terrorism Preparedness Coordinator for the Alameda County EMS Agency. Jim has a master’s degree in Homeland Security from the Naval Postgraduate School in Monterey, CA. He can be reached at jim.morrissey@acgov.org.
https://www.ems1.com/ems-education/articles/1482674-Tactical-EMS-An-overview/



 Active Shooter/Mass Casualty Incidents (AS/MCIs) in the U.S. have increased at an alarming rate in recent years. According to date collected by researchers at Texas State University, 47 active shootings events transpired between 2000 and 2008 — an average of 5.22 per year. Why should we be concerned? These figures have more than tripled in the past five years to an average of 16.8 annually, with a total of 89 active shooting incidents taking place between 2009 and 2013. There have also been disturbing trends in the scope and lethality of AS/MCIs. In the 2012 shootings in Aurora, Colorado, 70 people were wounded-12 fatally-when a gunman stormed the Century Theatre movie complex. Later that same year, 26 people, including 20 children, were murdered inside an elementary school in Newtown, Connecticut. And in April 2013, 264 people were injured in the Boston Marathon bombings, with 3 of the victims dying.
Active Shooter/Mass Casualty Incidents (AS/MCIs) in the U.S. have increased at an alarming rate in recent years. According to date collected by researchers at Texas State University, 47 active shootings events transpired between 2000 and 2008 — an average of 5.22 per year. Why should we be concerned? These figures have more than tripled in the past five years to an average of 16.8 annually, with a total of 89 active shooting incidents taking place between 2009 and 2013. There have also been disturbing trends in the scope and lethality of AS/MCIs. In the 2012 shootings in Aurora, Colorado, 70 people were wounded-12 fatally-when a gunman stormed the Century Theatre movie complex. Later that same year, 26 people, including 20 children, were murdered inside an elementary school in Newtown, Connecticut. And in April 2013, 264 people were injured in the Boston Marathon bombings, with 3 of the victims dying.
AS/MCIs present several dilemmas for public safety officials — the first of which is expediency of police response. There is a direct correlation between police response time and AS/MCI duration: the average AS/MCI lasts 12 minutes, with 37% ending in 5 minutes or less. Once police arrive on scene, the perpetrators typically turn their attention on police or commit suicide. Regardless, additional loss of life is usually mitigated upon police arrival and deployment on scene, as police prevent the assailants from accessing further victims.
Another notable problem manifested at AS/MCIs is the timeliness of emergency medical personnel response. In most instances, firefighter/paramedics are required to stay outside the secure perimeter while police clear the scene of the threat. This is a process that can take hours, as was the case with the Columbine and Washington Navy Yard shootings. While police search and neutralize active shooting scenes, those wounded desperately lay in wait for medical attention; a human being can die of blood loss in as little as 2-3 minutes, airway obstruction in 4-5 minutes, and a collapsed lung in 10 to 15 minutes. Therefore, paramedics need to be able to access and treat victims on scene, and cannot always wait for the police to conduct an exhaustive search for the perpetrators of active shootings.
In stark comparison to the rapid interdiction model implemented by police organizations across the U.S., most fire/EMS departments do not have established protocols for treating the wounded at active shooting events. The typical response is for fire personnel and paramedics to remain on standby until the scene has been rendered safe by police. Officials at some jurisdictions, such as the Arlington County Fire Department (ACFD), have s adopted a more proactive approach. In 2007, ACFD established the nation’s first Rescue Task Force (RTF). The RTF is based on the military’s Tactical Combat Casualty Care (TCCC) protocols. RTF consists of specially equipped firefighter paramedics partnered with police officers to respond to active shooter or other atypical, high threat medical emergencies. Other fire departments, such as those in Orange County and Los Angeles, California have also recently created Rescue Task Forces after active shooting events. Although the initiation of these RTFs is a positive development, the majority of municipalities in the U.S. do not have the standard operating procedures, equipment, or trained personnel to effectively deal with medical emergencies during active shooter and mass casualty incidents. It often takes a tragic event, such as the Los Angeles International Airport Shooting in November 2013, to demonstrate why Tactical Emergency Casualty Care (TECC) programs such as Rescue Task Forces are necessary.
Several prominent public safety organizations in the U.S. have recommended the establishment of formalized tactical emergency programs. The International Association of Firefighters (IAFF), a fire service advocacy group with over 300,000 members, has issued Position Statements recommending the establishment of TECC and Rescue Task Force programs. The Hartford Consensus, an ad-hoc group medical emergency professionals which includes representatives from the American College of Surgeons, fire service officials and Federal Bureau of Investigation (FBI) also recommends the adoption of Tactical Combat Casualty Care (TCCC) programs* by state and local public safety agencies. According to the Hartford Consensus, TCCC programs are quintessential in improving survivability of victims in active shooting events because they make provisions for “a more integrated response by law enforcement fire/rescue.”
In September 2013, the U.S. Fire Administration issued formal recommendation that public safety agencies across the U.S. look to TECC programs to provide optimal response to active shooter and mass casualty events: “Training, equipment and protocols around use of TECC for medical first responders should be explored, considered and implemented when feasible.”
The Committee-Tactical Emergency Casualty Care (C-TECCC), which is comprised of emergency medical experts from over 55 agencies, is working to expedite the transition of TCCC to the civilian domain. C-TECC recommends, and works with agencies all over the U.S. to advocate and assist with implementation of TECC programs.
Despite the declared need for tactical emergency medical programs by emergency medical professionals and public safety officials across the U.S., there exists no national standard or policy for the implementation of such programs. In fact, most jurisdictions in the U.S. currently have no standardized tactical emergency programs; if TECC programs are implemented, they are frequently established only after calamities involving loss of life occur. On a multi-jurisdictional level, there appears to be disconnect between identification of the problem, and realization of the solution to this problem.
Chances are, you live in an area that does not have a Rescue Task Force, or any other type of formalized TECC program. I would recommend that you engage your elected officials and public safety officials to see what the comprehensive plans are for response to a mass casualty event in your city or town. It is not a matter of if, but when your community will have to endure a mass casualty event.
*TCCC (Tactical Combat Casualty Care) is the original tactical emergency medical program created by the U.S. military, and TECC is the civilian off-shoot version of TCCC. Rescue Task Force (RTF) is a TECC-based program.

NIJ 06 Level IIIA Soft Armor Ballistic Protection
Front and back hard armor plate pockets able to receive multiple size plates
Mil-Spec industrial reinforced webbing
Front and back MOLLE modular attachment system (PALS compatible)
Durable 1,000-denier Cordura nylon external carrier construction
Adjustable hook and loop side straps – expandable up to 60”
Mil-Spec industrial reinforced webbing
Front and back MOLLE modular attachment system (PALS compatible)
Durable 1,000-denier Cordura nylon external carrier construction
Adjustable hook and loop side straps – expandable up to 60”
The Rescue Task Force Vest Kit combines state-of-the-art ballistic personal protection along with life-saving, battlefield proven medical equipment from North American Rescue. This ideal solution was designed for EMS, Fire-Rescue and Law Enforcement personnel performing medical operations in response to Active Shooter and Mass Casualty Incidents (AS/MCI).
Developed for rescue personnel working in the Direct and Indirect Threat areas of AS/MCI’s, the Rescue Task Force Vest Kit provides rescuers with a personal protective ballistic vest combined with the essential medical equipment to provide immediate point-of-wounding care to injured casualties in accordance to Tactical Emergency Casualty Care (TECC) guidelines.
The ballistic protective vest provides rescuers with one of the largest NIJ 0101.06 Level IIIA front/back panel soft armor protection systems available in the industry. The vest comes with built-in front and back hard armor plate pouches to allow the option to upgrade up to various sizes of Level IV hard plate protection. The ballistic soft armor is comprised of a unique, multi-hit capable, patent-pending assembly of ballistic materials that capture projectiles and disperse the energy over the entire surface of the panel. The kit is also available with the optional cummerbund-style side Level IIIA soft armor that also has an additional plate pouch to add hard plates for increased lateral protection. This full configuration offers Level IIIA soft armor front, back and side ballistic protection that has the capability to be upgraded with Level IV hard plates.
This “one-size-fits-most” soft armor ballistic vest easily adjusts at the shoulder and waist to fit different size rescuers. The front and back panels, shoulder straps and optional cummerbund side armor have MOLLE capability that allows for the attachment of additional medical or extraction equipment. Designed to address the top leading causes of potentially preventable death in a tactical environment, the medical equipment can also be modified to meet your agency’s needs as required by your protocols. Armor and medical products can also be purchased separately.
Special Features:
NIJ 06 Level IIIA Soft Armor Ballistic Protection
Front and back hard armor plate pockets able to receive multiple size plates
Optional cummerbund-style Side Armor Protection available with additional plate pouch
Mil-Spec industrial reinforced webbing
Front and back MOLLE modular attachment system (PALS compatible)
Durable 1,000-denier Cordura nylon external carrier construction
Adjustable hook and loop side straps – expandable up to 60”
Rescue Handle – 1,200 lbs. tensile strength reinforced strap
One of the largest soft armor coverage areas in the industry
Adjustable hook and loop padded shoulder straps with MOLLE plus two fixed “D” rings
5-year manufacturer’s warranty
Blast mitigation configuration
Comes complete with NAR-4 Chest Pouch with modified equipment list (see kit contents list) and additional CAT Tourniquets and CAT Holders
Made in the USA
Kit Contents:
1 x Armor, Tactical Responder Vest MKII
1 x Armor, Rescue Responder Side Set
4 x Combat Application Tourniquet – BLK
2 x Emergency Trauma Dressing – 6”
2 x S-Rolled Gauze
2 x NPA w/Lube – 28F
1 x HyFin® Vent Chest Seal Twin Pack
3 x Bear Claw Glove Kit (Pair) – Size Lg
1 x NAR Trauma Shears – 7-1/4”
1 x NAR Scissor Leash
4 x Combat Casualty Card
2 x Black Permanent Marker
2 x CAT Holder
1 x Bag, NAR-4 Chest Pouch
1 x MED Illuminous Patch
2 x Rescue Task Force Patch
Technical Specifications:
Complies with and exceeds NIJ Ballistic Resistance Standard 0101.06 for ballistic performance of Level IIIA body armor
Front, back and side hard armor plate pouches for increased protection (plates not included)
Front/back panel protection area: 187 sq. inches (11”W x 17”H)
Proprietary assembly of ballistic materials
Available Side Armor protection
Ballistic Vest Weight: Less than 13 lbs.
NIJ 06 Level IIIA Soft Armor Ballistic Protection
Front and back hard armor plate pockets able to receive multiple size plates
Optional cummerbund-style Side Armor Protection available with additional plate pouch
Mil-Spec industrial reinforced webbing
Front and back MOLLE modular attachment system (PALS compatible)
Durable 1,000-denier Cordura nylon external carrier construction
Adjustable hook and loop side straps – expandable up to 60”
Rescue Handle – 1,200 lbs. tensile strength reinforced strap
One of the largest soft armor coverage areas in the industry
Adjustable hook and loop padded shoulder straps with MOLLE plus two fixed “D” rings
5-year manufacturer’s warranty
Blast mitigation configuration
Comes complete with NAR-4 Chest Pouch with modified equipment list (see kit contents list) and additional CAT Tourniquets and CAT Holders
Made in the USA
Kit Contents:
1 x Armor, Tactical Responder Vest MKII
1 x Armor, Rescue Responder Side Set
4 x Combat Application Tourniquet – BLK
2 x Emergency Trauma Dressing – 6”
2 x S-Rolled Gauze
2 x NPA w/Lube – 28F
1 x HyFin® Vent Chest Seal Twin Pack
3 x Bear Claw Glove Kit (Pair) – Size Lg
1 x NAR Trauma Shears – 7-1/4”
1 x NAR Scissor Leash
4 x Combat Casualty Card
2 x Black Permanent Marker
2 x CAT Holder
1 x Bag, NAR-4 Chest Pouch
1 x MED Illuminous Patch
2 x Rescue Task Force Patch
Technical Specifications:
Complies with and exceeds NIJ Ballistic Resistance Standard 0101.06 for ballistic performance of Level IIIA body armor
Front, back and side hard armor plate pouches for increased protection (plates not included)
Front/back panel protection area: 187 sq. inches (11”W x 17”H)
Proprietary assembly of ballistic materials
Available Side Armor protection
Ballistic Vest Weight: Less than 13 lbs.

Tactical EMS
with Jim Morrissey
Active shooter: Rescue Task Force medics get to victims fasterRescue task forces and tactical medics offer different, yet more aggressive approaches to active-shooter incidents than standing by until all is clearJul 24, 2015
There have been two major shifts in doctrine related to law enforcement operations in the last 10 years. The first shift is the aggressive pursuit of an active shooter with whatever assets happen to be on hand instead of waiting for a SWAT team.
The second major change is recognizing the need for emergency medical contingency planning. This includes training all tactical personnel and line officers in the basics of self-care and buddy care with the focus on bleeding control and the addition of a dedicated tactical medic.
An aspect of this doctrine shift is SWAT teams are increasingly including a dedicated tactical medical component and medical threat assessment as part of their organizational structure. The result is a tactical medic being assigned to the law enforcement team using one of several models.
In addition, law enforcement is at minimum notifying — or ideally involving — local EMS and hospitals about planned or developing law enforcement operations that have a high risk for injuries, like an active shooter incident. This change has given rise to the rescue task force.
TACTICAL MEDIC VS. RESCUE TASK FORCE
Tactical medics are attached to and considered part of a tactical law enforcement team. Whereas a rescue task force is a trained, but hastily formed group of EMS medical providers (private and/or fire based) that partner with law enforcement on scene. They will enter a newly secured area, such as an active shooter incident, to provide triage, emergent care and casualty extrication.
Both tactical medics and rescue task force (RTF) personnel provide emergent care in less than ideal situations, often under significant stress and in chaotic, sometimes hostile environments. Both work very closely with law enforcement during planning, training and actual events.
Most RTF members are outfitted with ballistic vests and helmets, and likewise, almost without exception, tactical medics are protected with body armor and helmets. Both are specifically trained and equipped to deal with ballistic, blast and other violence-induced trauma.
RTF members wear their usual daily uniform (Fire/ EMS/ law enforcement) and are typically dispatched during their normal shift. Tactical medics wear the uniform of the tactical team they are attached to and are physically located with the team, or just outside of the hot zone.
RESCUE TASK FORCE MEDICS
Historically, EMS providers staged a safe distance away until police methodically secured the scene before permitting EMS to access victims. This practice is being phased out and replaced by the rescue task force, a more patient-centric and life-saving approach.
The RTF should have access to the wounded casualties when the threat has been eliminated, when the shooter is confined to another area, or when the scene has been deemed relatively secure. In the RTF model, providing life-saving interventions is done as soon as possible and is everyone's responsibility. There are four ways to render medical aid in these types of situations.
Bystanders and victims provide care to one another prior to any responder arrival.
Police rapidly extricate and escort victims to a safe area where awaiting EMS provides medical aid.
Police secure the area and provide life-saving interventions at the point of wounding.
Police secure or clear the area and bring in RTF medics under a force protection model.
The RTF focus should be on quick initial medical assessments and to provide life-saving interventions on scene, at the point of wounding or injury. Finding and treating patients should
be done in concert with efforts to extricate victims to a casualty collection point where a secondary triage, treatment and transport can be provided.
The RTF should use a pre-entry checklist to ensure important issues are addressed. The law enforcement job with the RTF is focused on escorting and protecting the medical members.
The RTF concept is becoming more widespread and adopted nationwide. However, fire departments, local EMS providers and law enforcement need to collaboratively train, drill and develop procedures and protocols for this concept to be effective.
TACTICAL MEDICS
A tactical medic is somewhat analogous to a professional sports team trainer who travels with the team and is there primarily to provide medical aid to the team, whether the injury or ailment is serious or not.
On a typical planned SWAT operation there are several phases and steps that take place well before the hit. Most often, the mission is a planned high-risk search or arrest warrant. After getting a warning order, the SWAT team operators and all of the support elements (medical, communications, negotiators, etc.) typically convene at a forward staging area.
A briefing will occur, where mission goals, subjects and target location layouts are reviewed. Depending on the nature of the mission and operations security issues, the tactical medic may coordinate with the local EMS transport provider to have an ALS ambulance stage close to the location.
The tactical medic is the logical liaison to the on-scene EMS assets that support law enforcement operations. Typically, the tactical medic will have a face-to-face meeting with EMS units.
The most common items dispensed by a tactical medic is bandages and over-the-counter pain relievers. However, the tactical medic must also be prepared to provide life-saving interventions to team members and other on-scene law enforcement officers.
The tactical medic will also provide initial medical care as needed to victims, bystanders, and perpetrators once the scene is secured. They will transfer patient care to a standard EMS unit if further care and transportation to the hospital is needed.
TACTICAL EMS MODELS
Some law enforcement agencies send personnel to EMT school or other comprehensive tactical medical classes. Those officers may become the default tactical medic for the team. That may be a workable solution; however, it is unlikely those individuals have the medical experience and patient-assessment skills needed to be the best medical practitioner in high-risk, high-stress situations.
There are countless workable models for the incorporation of a medical contingency plan for law enforcement operations. These are some of the more common models.
Officer, agent or trooper medic
A sworn law enforcement officer has dual roles as an operator and medic; they have law enforcement powers and can certainly protect themselves from potential threats.
Agency contract
The law enforcement agency has a contract or memorandum of understanding with a local EMS agency to provide up-close medical care. Some agencies put these contracted medics through a reserve officer school so that they can be armed as police.
Individual contract
An individual or a team are under contract or memorandum of understanding with the law enforcement agency for providing medical coverage for SWAT missions and training.
ALS stand by
In this outdated model, there are no tactical medics attached to the law enforcement team, but police will stage a standard ambulance some distance away to respond to the scene after the scene is secured by law enforcement.
LEARNING ABOUT TACTICAL EMS
Many in the EMS field have demonstrated an interest in getting into the field of tactical medicine. In addition to the pre-existing medical training, it is highly recommended to procure specific tactical medical education.
Programs such as NAEMT Tactical Combat Casualty Care (TCCC), Tactical Life Saver and others like have been well received by the EMS and LE community. The International School of Tactical Medicine offers a two-week intensive program aimed at medical practitioners who need basic training on law enforcement operations and how to work within a law enforcement team as the medic.
About the author
Jim Morrissey is a former Tactical Paramedic for the San Francisco FBI SWAT team and the founder of the Tactical Medical Association of California (TMAC). Jim is also the Terrorism Preparedness Coordinator for the Alameda County EMS Agency. Jim has a master’s degree in Homeland Security from the Naval Postgraduate School in Monterey, CA. He can be reached at jim.morrissey@acgov.org.

Asistencia de salud en peligro: la importancia de proteger al personal de salud en zonas de guerra PDF Gratis http://emssolutionsint.blogspot.com/2018/06/asistencia-de-salud-en-peligro-la.html

SERVICIOS PREHOSPITALARIOS Y DE AMBULANCIAS EN SITUACIONES DE RIESGO. PDF GRATIS http://emssolutionsint.blogspot.com/2018/06/servicios-prehospitalarios-y-de.html








Tactical and Disaster Medicine
with Dr. David K. Tan
Rescue Task Force is best medical response to an active shooter incidentThe EMS providers on the RTF focus on care of the victims while tactical medics focus on needs of the SWAT teamOct 9, 2015
Nearly six years after Arlington County Fire Department introduced the modern concept of the Rescue Task Force (RTF) model for emergency medical response to active shooter incidents, many agencies have yet to even discuss the topic, let alone begin training their personnel to mitigate this ever-increasing threat in our communities. A common reason offered for this lack of planning is, "Well, we have SWAT medics with tactical EMS training in our area that will respond."
Tactical Emergency Medical Support, or TEMS or SWAT medics, is certainly one option for managing multiple casualties in a high-threat environment, but having it as the only option for your community is less than optimal for two important reasons.
1. TEMS is for the SWAT team
The focus of TEMS providers is on the overall health and well-being of the SWAT team itself. Their mission is to protect the protectors by being immediately available for downed officers and to provide medical intelligence that may be of tactical value to command staff.
2. TEMS providers are a SWAT asset
Tactical medics do not deploy independently. They are a SWAT asset under SWAT command with a typical SWAT response time that far exceeds the typical duration of active killing that occurs during such incidents.
Rescue Task Force
The RTF model focuses on the needs and care of the victims of a mass shooting. RTF providers work with the first-arriving patrol officers to deliver immediate medical intervention for readily treatable injuries, like severe bleeding and airway compromise, which stabilizes victims for evacuation to definitive care.
RTF providers do not wait for police to secure the scene while victims lay bleeding to death inside the perimeter. They respond with police into the warm zone to find victims, even as other officers search for and neutralize the suspect.
Both TEMS and RTF have their place in the continuum of medical care when it comes to acts of active violence, but we must begin focusing on wider acceptance of RTF integration into police response to make any meaningful impact on morbidity and mortality when active shooter incidents occur.
About the author
David K. Tan, M.D., EMT-T, FAEMS, is associate professor and chief of EMS in the division of emergency medicine at Washington University School of Medicine in St. Louis. He is double board-certified in Emergency Medicine and EMS Medicine by the American Board of Emergency Medicine. Dr. Tan remains very active in EMS at the local, state and national levels as an operational medical director for local police, fire, and EMS agencies, Vice-chairman of the Missouri State Advisory Council on EMS, and President-Elect of the National Association of EMS Physicians. Dr. Tan is a member of the EMS1 Editorial Advisory Board. He also provides medical direction to EMS1.com and the EMS1 Academy.

RESCUE TASK FORCE RTF
Procedimiento Antiguo: , Bomberos (Paramedicos) responsables de hacer un Centro Medico de Triage a una distancia segura de los tiradores, mas conocida como ZONA FRIA, y espera hasta que la policia (Fuerzas de Seguridad" aseguren el area antes de tratar a las victimas (heridos)
Nuevas Tacticas: Paramedicos entraran a la "ZONA CALIENTE" con la policia, igualmente aun el tirador no ha sido contenido (Neutralizado) y aun la amenza persista.
Active Shooter/Mass Casualty Incidents (AS/MCIs) in the U.S. have increased at an alarming rate in recent years. According to date collected by researchers at Texas State University, 47 active shootings events transpired between 2000 and 2008 — an average of 5.22 per year. Why should we be concerned? These figures have more than tripled in the past five years to an average of 16.8 annually, with a total of 89 active shooting incidents taking place between 2009 and 2013. There have also been disturbing trends in the scope and lethality of AS/MCIs. In the 2012 shootings in Aurora, Colorado, 70 people were wounded-12 fatally-when a gunman stormed the Century Theatre movie complex. Later that same year, 26 people, including 20 children, were murdered inside an elementary school in Newtown, Connecticut. And in April 2013, 264 people were injured in the Boston Marathon bombings, with 3 of the victims dying.
AS/MCIs present several dilemmas for public safety officials — the first of which is expediency of police response. There is a direct correlation between police response time and AS/MCI duration: the average AS/MCI lasts 12 minutes, with 37% ending in 5 minutes or less. Once police arrive on scene, the perpetrators typically turn their attention on police or commit suicide. Regardless, additional loss of life is usually mitigated upon police arrival and deployment on scene, as police prevent the assailants from accessing further victims.
Active Shooter/Mass Casualty Incidents (AS/MCIs) in the U.S. have increased at an alarming rate in recent years. According to date collected by researchers at Texas State University, 47 active shootings events transpired between 2000 and 2008 — an average of 5.22 per year. Why should we be concerned? These figures have more than tripled in the past five years to an average of 16.8 annually, with a total of 89 active shooting incidents taking place between 2009 and 2013. There have also been disturbing trends in the scope and lethality of AS/MCIs. In the 2012 shootings in Aurora, Colorado, 70 people were wounded-12 fatally-when a gunman stormed the Century Theatre movie complex. Later that same year, 26 people, including 20 children, were murdered inside an elementary school in Newtown, Connecticut. And in April 2013, 264 people were injured in the Boston Marathon bombings, with 3 of the victims dying.
AS/MCIs present several dilemmas for public safety officials — the first of which is expediency of police response. There is a direct correlation between police response time and AS/MCI duration: the average AS/MCI lasts 12 minutes, with 37% ending in 5 minutes or less. Once police arrive on scene, the perpetrators typically turn their attention on police or commit suicide. Regardless, additional loss of life is usually mitigated upon police arrival and deployment on scene, as police prevent the assailants from accessing further victims.
Another notable problem manifested at AS/MCIs is the timeliness of emergency medical personnel response. In most instances, firefighter/paramedics are required to stay outside the secure perimeter while police clear the scene of the threat. This is a process that can take hours, as was the case with the Columbine and Washington Navy Yard shootings. While police search and neutralize active shooting scenes, those wounded desperately lay in wait for medical attention; a human being can die of blood loss in as little as 2-3 minutes, airway obstruction in 4-5 minutes, and a collapsed lung in 10 to 15 minutes. Therefore, paramedics need to be able to access and treat victims on scene, and cannot always wait for the police to conduct an exhaustive search for the perpetrators of active shootings.
In stark comparison to the rapid interdiction model implemented by police organizations across the U.S., most fire/EMS departments do not have established protocols for treating the wounded at active shooting events. The typical response is for fire personnel and paramedics to remain on standby until the scene has been rendered safe by police. Officials at some jurisdictions, such as the Arlington County Fire Department (ACFD), have s adopted a more proactive approach. In 2007, ACFD established the nation’s first Rescue Task Force (RTF). The RTF is based on the military’s Tactical Combat Casualty Care (TCCC) protocols. RTF consists of specially equipped firefighter paramedics partnered with police officers to respond to active shooter or other atypical, high threat medical emergencies. Other fire departments, such as those in Orange County and Los Angeles, California have also recently created Rescue Task Forces after active shooting events. Although the initiation of these RTFs is a positive development, the majority of municipalities in the U.S. do not have the standard operating procedures, equipment, or trained personnel to effectively deal with medical emergencies during active shooter and mass casualty incidents. It often takes a tragic event, such as the Los Angeles International Airport Shooting in November 2013, to demonstrate why Tactical Emergency Casualty Care (TECC) programs such as Rescue Task Forces are necessary.
Several prominent public safety organizations in the U.S. have recommended the establishment of formalized tactical emergency programs. The International Association of Firefighters (IAFF), a fire service advocacy group with over 300,000 members, has issued Position Statements recommending the establishment of TECC and Rescue Task Force programs. The Hartford Consensus, an ad-hoc group medical emergency professionals which includes representatives from the American College of Surgeons, fire service officials and Federal Bureau of Investigation (FBI) also recommends the adoption of Tactical Combat Casualty Care (TCCC) programs* by state and local public safety agencies. According to the Hartford Consensus, TCCC programs are quintessential in improving survivability of victims in active shooting events because they make provisions for “a more integrated response by law enforcement fire/rescue.”
In September 2013, the U.S. Fire Administration issued formal recommendation that public safety agencies across the U.S. look to TECC programs to provide optimal response to active shooter and mass casualty events: “Training, equipment and protocols around use of TECC for medical first responders should be explored, considered and implemented when feasible.”
The Committee-Tactical Emergency Casualty Care (C-TECCC), which is comprised of emergency medical experts from over 55 agencies, is working to expedite the transition of TCCC to the civilian domain. C-TECC recommends, and works with agencies all over the U.S. to advocate and assist with implementation of TECC programs.
Despite the declared need for tactical emergency medical programs by emergency medical professionals and public safety officials across the U.S., there exists no national standard or policy for the implementation of such programs. In fact, most jurisdictions in the U.S. currently have no standardized tactical emergency programs; if TECC programs are implemented, they are frequently established only after calamities involving loss of life occur. On a multi-jurisdictional level, there appears to be disconnect between identification of the problem, and realization of the solution to this problem.
Chances are, you live in an area that does not have a Rescue Task Force, or any other type of formalized TECC program. I would recommend that you engage your elected officials and public safety officials to see what the comprehensive plans are for response to a mass casualty event in your city or town. It is not a matter of if, but when your community will have to endure a mass casualty event.
*TCCC (Tactical Combat Casualty Care) is the original tactical emergency medical program created by the U.S. military, and TECC is the civilian off-shoot version of TCCC. Rescue Task Force (RTF) is a TECC-based program.
Credits https://medium.com/homeland-security/is-your-community-ready-for-an-active-shooter-event-66fb4000194d




Don’t Shoot! An Argument for Unarmed EMS
By Jody Marks, BS, RN, NRP Jul 17, 2017
There is an important discussion happening right now about whether EMS personnel should be armed. I have had conflicting feelings about this issue for years, but I think we’re fast approaching a tipping point, as the world of public safety seems to be growing more violent and tense. The November 2016 ambush of police officers in Iowa illustrates with sickening clarity the real danger of being vulnerable in a hostile world. Despite this inevitable risk and the legitimate points raised by advocates of armed EMS, however, becoming an armed first responder sounds like a bad idea to me.
A little personal background for context: I am not antigun. Both of my parents were police officers. I learned to shoot as soon as I was big enough to hold a firearm. I received a rifle for my birthday when I was in elementary school. I have held a concealed carry permit for years, and I typically carry a pistol either in my vehicle or on my hip when I am off duty. Plus, I live in Alabama. Firearms are as much a part of our culture as college football and sweet tea. Mostly nobody bats an eye around here when someone walks into a restaurant or store openly carrying a pistol.
For years before my time, my service allowed employees to carry firearms if they chose. My favorite EMS image of all time is a photo from the local newspaper (maybe circa 1980) showing a pioneer of EMS in our area crouched in the road at an accident scene with a gigantic revolver sticking out of his back pocket.
Their firearms policy at my service has since been eliminated, and we are no longer allowed to carry guns on duty. Nevertheless, within the larger local fire and EMS community, there remains a sort of unwritten “don’t ask, don’t tell” policy regarding firearms. I’m certain I’ve worked with armed partners on the ambulance at every service I’ve been with, but it’s not something that’s ever discussed in a professional setting in the absence of a close personal friendship. Lately I have noticed a few volunteers in more rural areas openly carrying pistols on calls, but the majority of responders I have been around seem to maintain the same sort of low-key attitude about the issue.
Despite my own familiarity with firearms and the generally permissive attitude about them in my area, I have never carried a gun on the ambulance with me. In no particular order, here are the reasons why:
1. In 18 years of EMS, I have never once found myself in a situation where I felt unsafe because I didn’t have a gun. In retrospect I cannot recall a single instance during my career about which I now think, I wish I had killed someone that day. I understand this is subject to change at any moment, and I understand that many others have not been so fortunate, but this is my experience.
2. I am not the police. I do not want to be the police. I do not want to look like the police or act like the police. I have no desire to fight with, detain, arrest, injure or kill anyone. I don’t like conflict. I don’t care about having authority or deciding who is right or wrong. I only want to help. Some EMS providers do seem to enjoy acting like the police. I recommend that these people actually become police officers or soldiers or MMA fighters so they can channel their aggression appropriately.
3. First do no harm—that’s us. I want my patients to trust me and think of me as someone who will help them regardless of their situation or what they may have done. It’s hard enough to gain people’s trust and convince them I really am trying to act in their best interest without them thinking I might decide to kill them.
4. I am not properly trained. I know how to aim and fire a gun, but I have no formal training on how to handle a gun in an actual fight. The odds of me being shot with my own gun are probably a lot higher than I would like to believe. Gun or no gun, someone with military or law enforcement training would likely still have the upper hand in a close altercation with me.
5. I am too busy to worry about protecting my gun. I am focused on treating my patient, not the things in my pockets or on my belt. Someone could easily snatch my pistol out of its holster while I’m engaged with a patient, and I might not even notice.
6. I don’t need another heavy, bulky, expensive thing to carry around.
7. Carrying a gun makes me think about shooting people. When I am carrying, I find myself constantly thinking about my weapon and the potential for using it rather than enjoying the day. When I’m at work I need to be focused on caring for people. I find it difficult to care much about someone I’m considering shooting.
8. I personally know or have met more than a few people (friends, relatives and patients) who have shot themselves accidentally or been shot accidentally by someone else. At least two-thirds of the gunshot wounds I have dealt with have been accidental. I have very little desire to shoot someone else. I have absolutely no desire to shoot myself or be shot by a coworker.
9. Carrying a gun gives me a sense of security that is likely at least partly false. Being armed might make me hesitate just a little bit less about going onto questionable scenes before law enforcement arrives. Singer Steve Earle makes this point nicely about his Colt revolver in his song “The Devil’s Right Hand”: “It’ll get you into trouble, but it can’t get you out.”
10. I think one of the best ways to stay safe when dealing with altered and/or violent patients is to simply avoid being seen as a threat. Public knowledge that we are armed or visibly carrying a firearm would take that little psychological advantage away from us.
Should we actually become armed or have the option of arming ourselves, it will create an interesting dilemma for those of us who prefer to remain unarmed. My decision would depend on the public’s awareness of the situation. If there was a story on the news or if my coworkers all started openly carrying firearms, I would feel obliged to do the same. I want to be an unarmed paramedic, not the unarmed paramedic. Bringing scissors to a gunfight is not a mistake I want to make. If people expect us to be armed, then we need to be armed. On the other hand, if we simply had an option to carry a concealed firearm, unknown to the public at large, I would feel much more comfortable remaining unarmed and letting my coworkers do the shooting.
Whatever dangers lurk out there for us, the fact remains that we are currently not expected to be armed, and thus any aggression directed toward us is almost automatically indefensible. If we arm ourselves, however, the line between savior and aggressor blurs, and we not only become much bigger targets but also subject to the same liability and burden of proof regarding lethal force faced by our counterparts in law enforcement. I don’t want to see a cell phone video of myself killing a person who turns out to be unarmed. I don’t want protestors at my door or riots occurring downtown because of my actions. I don’t want an ounce more liability than I already have. We already have enough to worry about, friends; we do not need this extra weight on our shoulders.
Whatever happens, I hope decisions about this issue will be carefully considered and weighed by the powers that be. This is not a subject to be taken lightly. The last thing we need is a misguided, hastily implemented firearm policy that ends up making our job even more dangerous than it already is.
Jody Marks, BS, RN, NRP, has been a paramedic for 14 years. He currently works as a registered nurse specializing in post-anesthesia care and is pursuing his nurse practitioner degree. He lives and works in Huntsville, Ala. https://www.emsworld.com/article/218146/dont-shoot-argument-unarmed-ems


















Certificado oficial 1.0v del curso TCC-LEFR Tactical Casualty Care for Law Enforcement and First Responder by Dr. Peter Pons, es marca registrada en EUA, tenemos autorizacion por escrito para instruir y certificar dicha formacion especifica para Policias y Guardias Civiles, nacido con la ayuda de los Servicios de Emergencias y el Metro SWAT de Denver, Colorado EUA.
http://emssolutionsint.blogspot.com.es/2017/09/curso-tcc-lefr-tactical-casualty-care_4.html
http://

{kind=link}
CONTOMS Counter Narcotic and Terrorism Operational MEDICAL SUPPPORT
El programa CONTOMS se inició en 1990 para satisfacer la necesidad de capacitación médica especializada y apoyar a las fuerzas del orden publico en operaciones especiales.
La aplicación de la ley sigue siendo una ocupación peligrosa. Un total de 1,466 agentes del orden público murieron en el cumplimiento de su deber durante los últimos 10 años, un promedio de una muerte cada 60 horas o 146 por año. Hubo 117 policías en cumplimiento del deber en 2014. En promedio, en la última década, se han registrado 58,930 agresiones contra las fuerzas del orden público cada año, lo que ha provocado 15,404 heridos. Nuestros propios datos sugieren que los miembros del Equipo SWAT corren un alto riesgo de sufrir lesiones, y que mantienen un índice de bajas tan alto como 9 por cada 1000 misiones de oficiales.
La aplicación de la ley y los servicios militares han reconocido desde hace tiempo que el apoyo médico a las operaciones especiales puede aumentar la probabilidad de éxito de la misión. Este tipo de apoyo requiere una experiencia única y adicional, que es complementaria a las calificaciones básicas de los proveedores de atención médica prehospitalaria. Los sistemas comunitarios de servicios médicos de emergencia (SEM) en los Estados Unidos y en el extranjero se desarrollaron para responder a las necesidades de pacientes individuales en situaciones controladas. Sin embargo, en algunos lugares, los técnicos en emergencias medicas capacitados para el rol dentro del Servicio de Soporte Contra-Terrorismo, han prestado servicio para apoyar la lucha contra el terrorismo, la interdicción de drogas y otras actividades de aplicación de la ley sin ningún tipo de capacitación adicional. Estas actividades se han vuelto de naturaleza cada vez más especializadas, caracterizadas por operaciones prolongadas, fuerzas opositoras organizadas, uso de armas de tipo militar, muertes y lesiones cada vez mayores entre los agentes del orden público, los perpetradores y ciudadanos inocentes.
The CONTOMS Program was started in 1990 to meet the need for specialized medical training to support law enforcement special operations.
Law enforcement remains a dangerous occupation. A total of 1,466 law enforcement officers died in the line of duty during the past 10 years, an average of one death every 60 hours or 146 per year. There were 117 law enforcement officers killed in the line of duty in 2014. On average, over the last decade, there have been 58,930 assaults against law enforcement each year, resulting in 15,404 injuries. Our own data suggests that SWAT Team members are at high risk for injury, sustaining a casualty rate as high as 9 per 1000 officer-missions.
Law enforcement and the military services have long recognized that medical support of special operations can enhance the probability of mission success. This type of support requires a unique, additional expertise, which is complementary to the basic qualifications of prehospital health care providers. Community emergency medical services (EMS) systems in the United States and abroad were developed to respond to the needs of individual patients in controlled situations. However, in some locales, emergency medical technicians trained for the EMS role have been pressed into service to support counter terrorism, drug interdiction and other law enforcement activities without any additional training. These activities have become increasingly specialized in nature, characterized by prolonged operations, organized opposing forces, use of military-type weapons, and increasing death and injury among law enforcement officers, perpetrators and innocent citizens.

TACTICAL MEDIC HANDBOOK 2013 Edition. CONTOMS Counter Narcotic and Terrorism Operational MEDICAL SUPPPORT




What is Tactical Emergency Casualty Care? by CTECC
Tactical Emergency Casualty Care (TECC) is a set of evidenced-based and best practice trauma care guidelines for civilian high-threat pre-hospital environments. The TECC guidelines are built upon the critical medical lessons learned by US and allied military forces over the past 15 years of conflict and codified in the doctrine of Tactical Combat Casualty Care (TCCC). Using the military TCCC guidelines as a starting point, the Committee creates the civilian high threat medical guidelines through a process of literature research, evidence evaluation, expert discussion, and civilian best practices review. The TECC guidelines are built upon the foundations of TCCC but are different to meet the unique needs of the civilian medical and operational environments. The differences address civilian specific language, provider scope of practice, population, civilian liability, civilian mission and operational constraints, logistics, and resource acquisition.
How are TECC and TCCC similar?
Tactical Emergency Casualty Care is a set of civilian medical guidelines for high threat operations. Tactical Combat Casualty Care is a set of military medical guidelines for care of the wounded during military combat operations. The two sets of guidelines are naturally related, but each with a necessary difference in language, scope, applicability and flexibility.
There are two key unifying principles of TCCC and TECC. First is the process of guideline development. Both Committees are comprised of medics, physicians, academics and operational leaders. Both Committees began with prior operational and medical lessons learned- for CoTCCC this was Vietnam and Somalia, for C-TECC this was TCCC and OIF/OEF- and rapidly evolved their recommendations based on immediate lessons learned. Second is an understanding that success requires developing and deploying a SYSTEM of care. In the military, TCCC’s success fundamentally lies in the fact that all personnel deploying to a combat theater were trained in the principles of TCCC. The operational and trauma care systems were built around this training.
This second fact is also the main limiting factor for the deployment of TCCC in the civilian setting. As a system, TCCC cannot be deployed in the civilian setting because many recommendations run counter to civilian scope of practice and medical standards (e.g. use of hextend for resuscitation, pre-hospital antibiotics, needle decompression practiced by non medical personnel, etc.).
Version 1
How are TECC and TCCC different?
Tactical Emergency Casualty Care is the civilian evolution and application of the military Tactical Combat Casualty Care guidelines. When discussing the differences between the two, it is important to emphasize that TECC and TCCC are not in competition with each other; although, as the pictures from the recent Boston Marathon bombing demonstrate, the bullets and explosives may be similar in civilian settings as in military combat, this does not make the military guidelines directly applicable for civilian applications.
The two sets of guidelines are naturally related, but each with a necessary difference in language, scope, applicability and flexibility. There are three primary differences between TECC and TCCC: guideline terminology, trauma care recommendations and operational focus.
Terminology/ Language: TCCC was written by the military special operations community to specifically address the specificities and conditions surrounding combat operations. These guidelines are researched, developed, and written with the assumption that the patient is an otherwise healthy 18-45yo soldier and that the provider is working under the military defined scope of practice. The TCCC guidelines assume a military medical support system, military rules of engagement, and military legal precedent. While individual recommendations such as tourniquet use are valid, TCCC as a system has limited application in the civilian setting. The TCCC courses currently being taught were not intended for civilian application. The Pre-Hospital Trauma Life Support TCCC course comes from the military PHTLS textbook, a version that was specifically written for the military medical community because the civilian PHTLS textbook had a different focus and application.
All leaders with operational experience understand that the language changes in TECC are critical. As with the Incident Command System (ICS), common operating language is important for interagency response to complex threats. For example, “Care Under Fire”, has variable meanings across the Fire (e.g. actual fire), EMS (e.g. fire or gunshots- but a non operational zone) and Law Enforcement (e.g. active gunfire in the area) communities. Tactical Emergency Casualty Care was created to address these system limitations and specific scope of practice challenges related to TCCC. The C-TECC members, many of whom are active and past CoTCCC members, worked with civilian leaders to codify threat based guidelines (the core of TCCC) in a way that was easily applicable to civilian operations, legal and liability limitations and scope of practice, and in a way that is broadly applicable to the entirety of the civilian patient population.
Trauma care guidelines: TECC and TCCC trauma recommendations are closely related. TECC places less emphasis on pre-hospital antibiotics, hextend as a resuscitation fluid, and specific product solutions. The TECC guidelines place more emphasis on interagency communication, integrated operations between EMS, Fire and Law Enforcement, casualty extraction and evacuation, and care of non-combatant civilians. Additionally, as the civilian high threat focus continues with the results of on-going study and medical data, the recommendations of TECC will necessarily diverge in small ways from TCCC. One recent example is the 2013 pediatric TECC guidelines. Children are not accounted for in the TCCC guidelines as they are not in the military deployable population. As such, the C-TECC specifically examined the research and data specific to the pediatric population and created a specific set of recommendations for children.
Operational: The fundamental mission difference between the military and civilian high threat operations is important. In general, military operations focus on clearing, holding, and/or gaining territory with an emphasis on domination of enemy forces. By definition, civilian operations are rescue operations with the key missions of limiting civilian morbidity and mortality. Civilian first responders are sworn to “serve and protect”. Any guidelines must acknowledge this important difference and account for rescue operations, limitations in use of force, and other regional operational requirements.
How can I get certified in TECC?
The TECC guidelines are open source and non-proprietary with the exception of the TECC logo. There are currently no “official TECC courses” or a certified TECC provider/instructor.
The C-TECC believes that, though there are universal “principles” of high threat response, the application must be tailored for individual agencies based upon local resources, political climate, budget and operational experience. “Cookie cutter” or standardized courses and applications for high threat operations fail to account for the differences among first responders that vary widely jurisdiction to jurisdiction, region to region, state to state, etc. As such, the concepts and skills in these classes have to be ‘un-learned’ or ‘ignored’ because they do not fit into the specific agency SOP or scope.
TECC is not dogma, and the principles are meant to be applied uniquely by each agency that uses it, depending on that agency's provider levels, scope of practice, culture, patient population, risk assessment, etc. We consider the TECC guidelines to be a pile of bricks; take only the bricks that fit into your operational culture and build a response program that is unique to you. Just don’t change the individual bricks! Overall, the principles of TECC are not difficult to teach – the actual medical interventions such as pressure dressings and tourniquets are now commonplace for everyday trauma. What is unique about high threat medical principles is less about what is done medically and more about when it is done, what injuries on focused on, and what can be excluded.
There are training entities that offer TECC courses. The Committee does not require any of these as your application of TECC is unique to your agency. If you cannot develop your own training, several of these companies offer a solid foundation of training. In the future, those companies and institutions that meet the principles of TECC guidelines instruction as set forth by the Committee may display a special C-TECC logo and be listed on the C-TECC.org website; until then, if you take a TECC class, make sure you check into the background and experience of the instructors first, and make sure that they are not teaching you TCCC and calling it TECC!
How can I become a TECC instructor?
There is currently no C-TECC sanctioned certification or classification as a ‘TECC instructor.” If you have the operational and educational experience to teach in your agency, if you have experience as an educator, or you are recognized by your agency as an instructor, you can take the open source TECC guidelines and create a course of instruction specific to your agency’s SOPs.
I am a certified TCCC instructor. Can I teach TECC?
Sure, although it is certainly not required. Knowledge of TCCC is helpful as TCCC is the starting point for TECC. You must understand however that the two are not the same, and must be clear on the differences between the two. Please also refer to the TECC skill set; at no point should skills outside of scope of practice be taught to students as a part of TECC. For example, although TECC includes needle decompression of a chest, this skill set should NOT be taught to providers if it is not specifically included in their scope of practice. Other than that, if you are familiar with instruction of the military combat medical guidelines, then your understanding of how to instruct the civilian high threat medical guidelines should be solid!
How can my department or agency start a TECC program?
Implementing the TECC guidelines into your agency’s standard operations for high threat response is not as ‘heavy a lift’ or difficult as one would think. If you have an operational plan for deployment of assets and operations during situations of high threat, the medical guidelines will fit in easily. The individual TECC guidelines, such as applying a tourniquet or using hemostatic gauze, are becoming common place in everyday pre-hospital management of trauma. Remember that TECC is less about what you do and more about when you do it. Teaching the TECC guidelines to your agency should be done in a way that is specific to your agency’s culture, scope, and approach to operational training.
The Committee for Tactical Emergency Casualty Care is committed to assisting all response agencies and first responders who wish to utilize the guidelines. We have, and are working on, a variety of resources to assist you. Currently, we can provide a variety of educational articles and plenty of advice on how to get started. In the near future, we will be distributing a standard slide deck to get you started in teaching the guidelines. Feel free to contact the Committee with any questions or request for assistance.
Is TECC only for law enforcement and SWAT operations?
Absolutely not!!! Yes, it does have the word ‘tactical’ in its name but do not think that implies that the guidelines are for use only in law enforcement or tactical medical operations. Although the word ‘tactical’ in common use implies law enforcement associated operations, every first responder utilizes ‘tactics’ on every call every day. The Committee uses the word tactical to refer to the operational decisions that are made during response. Every one of these operational decisions has an effect on medical care and the competing priorities of operations and medical care need to be considered in real time. TECC allows you to do just this.
TECC has applications for ALL high risk operations, where there is a real and on-going risk to both the patient and provider. Examples of high risk operations include, but are not limited to:
Tactical Emergency Casualty Care (TECC) is a set of evidenced-based and best practice trauma care guidelines for civilian high-threat pre-hospital environments. The TECC guidelines are built upon the critical medical lessons learned by US and allied military forces over the past 15 years of conflict and codified in the doctrine of Tactical Combat Casualty Care (TCCC). Using the military TCCC guidelines as a starting point, the Committee creates the civilian high threat medical guidelines through a process of literature research, evidence evaluation, expert discussion, and civilian best practices review. The TECC guidelines are built upon the foundations of TCCC but are different to meet the unique needs of the civilian medical and operational environments. The differences address civilian specific language, provider scope of practice, population, civilian liability, civilian mission and operational constraints, logistics, and resource acquisition.
Tactical Emergency Casualty Care is a set of civilian medical guidelines for high threat operations. Tactical Combat Casualty Care is a set of military medical guidelines for care of the wounded during military combat operations. The two sets of guidelines are naturally related, but each with a necessary difference in language, scope, applicability and flexibility.
There are two key unifying principles of TCCC and TECC. First is the process of guideline development. Both Committees are comprised of medics, physicians, academics and operational leaders. Both Committees began with prior operational and medical lessons learned- for CoTCCC this was Vietnam and Somalia, for C-TECC this was TCCC and OIF/OEF- and rapidly evolved their recommendations based on immediate lessons learned. Second is an understanding that success requires developing and deploying a SYSTEM of care. In the military, TCCC’s success fundamentally lies in the fact that all personnel deploying to a combat theater were trained in the principles of TCCC. The operational and trauma care systems were built around this training.
This second fact is also the main limiting factor for the deployment of TCCC in the civilian setting. As a system, TCCC cannot be deployed in the civilian setting because many recommendations run counter to civilian scope of practice and medical standards (e.g. use of hextend for resuscitation, pre-hospital antibiotics, needle decompression practiced by non medical personnel, etc.).
Version 1
Version 2
Version 3
How are TECC and TCCC different?
Tactical Emergency Casualty Care is the civilian evolution and application of the military Tactical Combat Casualty Care guidelines. When discussing the differences between the two, it is important to emphasize that TECC and TCCC are not in competition with each other; although, as the pictures from the recent Boston Marathon bombing demonstrate, the bullets and explosives may be similar in civilian settings as in military combat, this does not make the military guidelines directly applicable for civilian applications.
The two sets of guidelines are naturally related, but each with a necessary difference in language, scope, applicability and flexibility. There are three primary differences between TECC and TCCC: guideline terminology, trauma care recommendations and operational focus.
Terminology/ Language: TCCC was written by the military special operations community to specifically address the specificities and conditions surrounding combat operations. These guidelines are researched, developed, and written with the assumption that the patient is an otherwise healthy 18-45yo soldier and that the provider is working under the military defined scope of practice. The TCCC guidelines assume a military medical support system, military rules of engagement, and military legal precedent. While individual recommendations such as tourniquet use are valid, TCCC as a system has limited application in the civilian setting. The TCCC courses currently being taught were not intended for civilian application. The Pre-Hospital Trauma Life Support TCCC course comes from the military PHTLS textbook, a version that was specifically written for the military medical community because the civilian PHTLS textbook had a different focus and application.
All leaders with operational experience understand that the language changes in TECC are critical. As with the Incident Command System (ICS), common operating language is important for interagency response to complex threats. For example, “Care Under Fire”, has variable meanings across the Fire (e.g. actual fire), EMS (e.g. fire or gunshots- but a non operational zone) and Law Enforcement (e.g. active gunfire in the area) communities. Tactical Emergency Casualty Care was created to address these system limitations and specific scope of practice challenges related to TCCC. The C-TECC members, many of whom are active and past CoTCCC members, worked with civilian leaders to codify threat based guidelines (the core of TCCC) in a way that was easily applicable to civilian operations, legal and liability limitations and scope of practice, and in a way that is broadly applicable to the entirety of the civilian patient population.
Trauma care guidelines: TECC and TCCC trauma recommendations are closely related. TECC places less emphasis on pre-hospital antibiotics, hextend as a resuscitation fluid, and specific product solutions. The TECC guidelines place more emphasis on interagency communication, integrated operations between EMS, Fire and Law Enforcement, casualty extraction and evacuation, and care of non-combatant civilians. Additionally, as the civilian high threat focus continues with the results of on-going study and medical data, the recommendations of TECC will necessarily diverge in small ways from TCCC. One recent example is the 2013 pediatric TECC guidelines. Children are not accounted for in the TCCC guidelines as they are not in the military deployable population. As such, the C-TECC specifically examined the research and data specific to the pediatric population and created a specific set of recommendations for children.
Operational: The fundamental mission difference between the military and civilian high threat operations is important. In general, military operations focus on clearing, holding, and/or gaining territory with an emphasis on domination of enemy forces. By definition, civilian operations are rescue operations with the key missions of limiting civilian morbidity and mortality. Civilian first responders are sworn to “serve and protect”. Any guidelines must acknowledge this important difference and account for rescue operations, limitations in use of force, and other regional operational requirements.
How can I get certified in TECC?
The TECC guidelines are open source and non-proprietary with the exception of the TECC logo. There are currently no “official TECC courses” or a certified TECC provider/instructor.
The C-TECC believes that, though there are universal “principles” of high threat response, the application must be tailored for individual agencies based upon local resources, political climate, budget and operational experience. “Cookie cutter” or standardized courses and applications for high threat operations fail to account for the differences among first responders that vary widely jurisdiction to jurisdiction, region to region, state to state, etc. As such, the concepts and skills in these classes have to be ‘un-learned’ or ‘ignored’ because they do not fit into the specific agency SOP or scope.
TECC is not dogma, and the principles are meant to be applied uniquely by each agency that uses it, depending on that agency's provider levels, scope of practice, culture, patient population, risk assessment, etc. We consider the TECC guidelines to be a pile of bricks; take only the bricks that fit into your operational culture and build a response program that is unique to you. Just don’t change the individual bricks! Overall, the principles of TECC are not difficult to teach – the actual medical interventions such as pressure dressings and tourniquets are now commonplace for everyday trauma. What is unique about high threat medical principles is less about what is done medically and more about when it is done, what injuries on focused on, and what can be excluded.
There are training entities that offer TECC courses. The Committee does not require any of these as your application of TECC is unique to your agency. If you cannot develop your own training, several of these companies offer a solid foundation of training. In the future, those companies and institutions that meet the principles of TECC guidelines instruction as set forth by the Committee may display a special C-TECC logo and be listed on the C-TECC.org website; until then, if you take a TECC class, make sure you check into the background and experience of the instructors first, and make sure that they are not teaching you TCCC and calling it TECC!
How can I become a TECC instructor?
There is currently no C-TECC sanctioned certification or classification as a ‘TECC instructor.” If you have the operational and educational experience to teach in your agency, if you have experience as an educator, or you are recognized by your agency as an instructor, you can take the open source TECC guidelines and create a course of instruction specific to your agency’s SOPs.
I am a certified TCCC instructor. Can I teach TECC?
Sure, although it is certainly not required. Knowledge of TCCC is helpful as TCCC is the starting point for TECC. You must understand however that the two are not the same, and must be clear on the differences between the two. Please also refer to the TECC skill set; at no point should skills outside of scope of practice be taught to students as a part of TECC. For example, although TECC includes needle decompression of a chest, this skill set should NOT be taught to providers if it is not specifically included in their scope of practice. Other than that, if you are familiar with instruction of the military combat medical guidelines, then your understanding of how to instruct the civilian high threat medical guidelines should be solid!
How can my department or agency start a TECC program?
Implementing the TECC guidelines into your agency’s standard operations for high threat response is not as ‘heavy a lift’ or difficult as one would think. If you have an operational plan for deployment of assets and operations during situations of high threat, the medical guidelines will fit in easily. The individual TECC guidelines, such as applying a tourniquet or using hemostatic gauze, are becoming common place in everyday pre-hospital management of trauma. Remember that TECC is less about what you do and more about when you do it. Teaching the TECC guidelines to your agency should be done in a way that is specific to your agency’s culture, scope, and approach to operational training.
The Committee for Tactical Emergency Casualty Care is committed to assisting all response agencies and first responders who wish to utilize the guidelines. We have, and are working on, a variety of resources to assist you. Currently, we can provide a variety of educational articles and plenty of advice on how to get started. In the near future, we will be distributing a standard slide deck to get you started in teaching the guidelines. Feel free to contact the Committee with any questions or request for assistance.
Is TECC only for law enforcement and SWAT operations?
Absolutely not!!! Yes, it does have the word ‘tactical’ in its name but do not think that implies that the guidelines are for use only in law enforcement or tactical medical operations. Although the word ‘tactical’ in common use implies law enforcement associated operations, every first responder utilizes ‘tactics’ on every call every day. The Committee uses the word tactical to refer to the operational decisions that are made during response. Every one of these operational decisions has an effect on medical care and the competing priorities of operations and medical care need to be considered in real time. TECC allows you to do just this.
TECC has applications for ALL high risk operations, where there is a real and on-going risk to both the patient and provider. Examples of high risk operations include, but are not limited to:
- Active shooter response
- Wilderness medicine
- Confined space, rope and other technical rescue operations
- Law enforcement ‘officer down’ response
- SWAT medical support
- Response to explosive mass casualty
- All other mass casualty response
How can I become involved with the Committee?
The development of the TECC guidelines was a grassroots effort by a group of operational medical personnel who identified the gap when applying military medical guidelines to a non-military population and operation. We remain a grassroots effort and thus all of our meetings are open to the public and everything we produce is available to all at no charge.
Anyone can participate in the discussion regarding the TECC guidelines. We want your opinions and involvement as the guidelines are intended for all to use, not for just a few with special “certifications.’ We have two meetings a year: every December in conjunction with the Special Operations Medical Association conference in Tampa, FL, and a spring meeting at a different location every year. As a whole, about two months prior, we publish the information and logistics for our next meeting on the C-TECC website.
As a 501c3, we have bylaws that outline the different committees, the number of members on each committee, the requirements for members and the process by which one becomes an official member. Part of that process is attending at least one meeting in person. If you are interested in becoming an official member, feel free to attend a meeting, and then contact us directly and submit a CV. In the meantime, be a part of the grassroots that is our foundation. Submit comments and questions on line – all will be heard and considered!
Are the Committee’s meetings open to the public?
As discussed in the question regarding how to become a member, all Committee meetings are open to the public. TECC is founded on a grassroots effort to address the operational gap that exists in high threat medical operations; as such, we want and encourage your opinions and involvement.
We have two meetings a year: every December in conjunction with the Special Operations Medical Association conference in Tampa, FL, and a spring meeting at a different location every year. As a whole, about two months prior, we publish the information and logistics for our next meeting on the C-TECC website.
How can I get more information on the Committee?
Just ask! We will do all we can to answer your questions and support your operational use of the TECC guidelines. Currently on our website, under the resources tab, there are several articles on TECC and C-TECC that you can access.
Are there approved TECC courses?
Currently, there is no course approval or certification for TECC. As a whole, you do not need a course in TECC. We recommend that you use the in-house training staff and operational experts in your agency to create an operational paradigm and training program that is specific to your agency. That being said, there are many companies and training programs that state they teach TECC courses. Many of these are very good, but several teach military TCCC and just call it TECC. The two sets of guidelines are similar and related, but definitely different! So, if you cannot do it in-house for whatever reason and instead are seeking a TECC course, buyer beware! Do your due diligence to ensure that the content is consistent with TECC guidelines, that the instruction is matched to the students scope of practice, and that the instructional cadre has the expertise and TECC experience that they claim. In the near future, companies that agree to meet and adhere to the principles of TECC guidelines instruction being created by the Committee will be able to display a special C-TECC logo and be listed on our website to denote that the course of instruction is consistent with the TECC guidelines.
How can I get my TECC course approved?
Currently there is no ‘course approval’ process for TECC instruction. Feel free to create your TECC course utilizing the TECC guidelines as they are written. However, you must adhere to the principles of TECC – do not teach procedures outside of your student’s scope of practice, do not refer to equipment or supplies as ‘approved’ or ‘preferred’ or ‘recommended’, and do not change the language or intent of the guidelines.
In the near future, the Committee will have a simple ‘principles of guidelines instruction’ that is an agreement between the Committee and the educational entity that will allow the course to display a special C-TECC logo to denote proper use and instruction of the guidelines.
What equipment is TECC approved?
None! The civilian patient population, the supply and equipment acquisition process, the budget and logistics of civilian response agencies and providers is completely different than the military. Just because a product is used or recommended by the military does NOT mean it is the best for civilian use. The military ‘recommended’ products are just that, recommended for the military population. These products do not take into account the aspects of civilian use including body and limb size, anticoagulation profiles, resources available, and the need for open bid acquisition.
The Committee also will not endorse products as such endorsements may be misconstrued as unethical or done with impropriety. The C-TECC will discuss and offer existing evidence for products that have been tested and demonstrated effective, but does not specifically endorse any product.
We recommend that every agency should explore the different product solutions available and make an agency specific decision based on available unbiased scientific data as well as agency and provider preference.
Why are so many TCCC courses being taught to civilians?
Tactical Combat Casualty Care is a great military medical innovation. These concepts have saved countless lives on the battlefield, and have provided a wealth of medical data for us to build upon. Until 2011, TCCC was the only existing set of high threat medical guidelines that existed. Multiple courses were developed to teach military personnel; these courses were made available to civilians as well.
What is interesting, however, is that even prior to the development of TECC from the TCCC guidelines, civilian personnel who were trained in TCCC through these standard courses would bring the concepts back and have to alter or change what they were taught to fit the constraints of the civilian application. Essentially, what was being done was these civilian providers were taking TCCC and making into something appropriate for civilians. This is exactly how the efforts of the Committee for Tactical Emergency Casualty Care began, and is exactly what we have codified in the TECC guidelines.
Courses in TCCC are still being offered and taught to civilians mainly because the infrastructure exists to do so; and these students are likely going back and changing what they learned to civilian appropriate for their agencies and application. As TECC continues to grow, the Committee will continue to distribute and emphasize the need for civilian specific and appropriate training through partnerships with federal agencies, civilian training entities such as PHTLS and ITLS, and future collaboration with professional pre-hospital, operational, and medical organizations.
How are the guidelines updated?
The Committee meets twice a year to discuss the guidelines and make changes based on current research and data. At these meetings, we review current research, data, and case reports that are relevant to the guidelines and raise questions as to where and what changes need to be made.
As a whole, the December full committee meeting opens the discussion on any aspect of the guidelines and sets agenda for discussion and voting for the spring full committee meeting. If overwhelming data becomes available in-between meetings that show that the application of any individual guideline could cause harm, the Board of Directors will consider and make the necessary changes in real-time with the input of the Guidelines Committee and our Board of Advisor experts. An example of this process was the changes made to the TECC guidelines regarding limiting the use of Hextend after the FDA’s warning on Hextend use in critically injured patients.
How can I submit a comment or an article for consideration?
Please by all means submit the reference through the website! We rely on all of the first response community to assist us in identifying relevant data and research that may affect the Guidelines.
How did TECC come to be included in the HSGP National Priorities, and how is it related to MCI preparedness?
Recent events such as the mass shootings in Aurora (CO), Newtown (CT) and the bombing at the Boston Marathon have solidified the recognition that a national capability gap exists in terms of pre-hospital trauma care. The life safety of our citizens is recognized as government’s highest duty, and FEMA has named MCI preparedness as a national priority in order to address this gap. Improved out-of-hospital trauma care is integral to the successful management of mass casualty events.
How did the TECC guidelines come about?
The Committee for Tactical Emergency Casualty Care (C-TECC) was formed in 2010 to formally translate military trauma lessons learned into the civilian high-threat pre-hospital community. The C-TECC is modeled after the highly successful Committee on Tactical Combat Casualty Care (CoTCCC) – frequently credited as one of the major initiatives that has resulted in the lowest combat mortality rates in modern history.
C-TECC brings together SME’s from EMS, fire, law enforcement and DHS/FEMA, as well as physicians from emergency departments, trauma centers and the military to develop evidence-based, best-practice principles of high-threat pre-hospital medicine.
What does TECC address that other guidelines do not?
The TECC guidelines take into account the requirements of a civilian population. This includes pediatric, geriatric, and special needs patients, as well as considerations for underlying medical conditions common in a civilian population, the characteristics and limitations of civilian EMS, and the varied types of threats that responders face.
Military treatment guidelines were developed for a very specific purpose and population – fit and healthy 18-45 year olds in a combat environment. They have been extremely successful, but these guidelines cannot be directly carried over into the civilian population without taking these differences into account.
Medic with GUNS
https://emssolutionsint.blogspot.com/2019/06/medics-with-guns.html
Is this a training curriculum or an equipment product line that is being marketed?
No – the TECC initiative was undertaken in order to advance the practice of trauma care in the pre-hospital civilian environment. To accomplish this, the guidelines are freely available to all. Training and equipment vendors are encouraged to incorporate the principles of TECC into their curricula and products.
C-TECC is a not-for-profit (501c3) organization composed of subject matter experts who volunteer their time in order to benefit the public. C-TECC doesn’t offer training courses or product lines, nor does it endorse specific vendors or products.
Does FEMA or any other federal agencies support or endorse TECC?
Several federal agencies (including FEMA, DHS–Office of Health Affairs and multiple federal law enforcement agencies) have a role in the work of C-TECC, and representation on the Committee. TECC is prominently featured in the Joint Counter Terrorism Workshop Series (JCTAWS) initiative, which helps prepare urban areas for major mass casualty events.
In order to support the efforts of implementing TECC into response paradigms, the FEMA Office of Counter Terrorism and Security Preparedness is sponsoring one-day seminars conducted by Technical Assistance teams composed of members from the C-TECC. The seminar is focused on providing an executive briefing on the development and uses of the guidelines, application design into existing and new response protocols, curriculum design and implementation strategies, and instructor train-the-trainer information.
FLORIDA BILL WOULD ALLOW PARAMEDICS TO CARRY GUNS WHEN RESPONDING TO MASS SHOOTINGS AT SCHOOLS BY JENNI FINK ON 3/26/19 AT 11:06 AM EDT
https://www.newsweek.com/florida-bill-would-allow-paramedics-carry-guns-when-responding-mass-shootings-1375429
How can my jurisdiction or agency get more information or an orientation to the TECC initiative?
The Committee is working on development of an orientation program that explains the foundations of the TECC principles, describes the medical evidence behind the guidelines and offers tips for implementation and training.
http://www.c-tecc.org/about/faq
Rescue Task Force RTF? / FUERZAS de TAREA de RESCATE. TEMS vs EMS
http://emssolutionsint.blogspot.com/2018/03/tactical-medics-vs-rescue-task-force.html
Uso del Torniquete de Emergencia TIE "TORNQUETE ESPAÑOL" by Manzanal Mampel
100% Europeo CE.

Free DOWNLOAD pdf
https://emssolutionsint.blogspot.com/2018/10/rescue-task-force-best-practices-guide.html
Mas temas y Documentos gratuitos sobre Medicina Tactica
http://emssolutionsint.blogspot.com/2018/07/medicina-tactica-pdf-videos-manuales.html


TELEGRAM Sociedad Iberoamericana de Emergencias https://t.me/joinchat/GRsTvEHYjNLP8yc6gPXQ9Q
Dr Ramon REYES, MD,
Por favor compartir nuestras REDES SOCIALES @DrRamonReyesMD, así podremos llegar a mas personas y estos se beneficiarán de la disponibilidad de estos documentos, pdf, e-book, gratuitos y legales..
Grupo Biblioteca/PDFs gratis en Facebook
https://www.facebook.com/groups/PDFgratisMedicina #DrRamonReyesMD
Facebook
Instagram
Pinterest
LinkedIn
Twitter
Blog
TELEGRAM