A 16-year-old football player presents to the emergency department directly from a game. He was tackled, falling onto his right shoulder. The patient is complaining of right-sided chest pain. On exam, there is tenderness over the right sternoclavicular joint (SCJ) with a prominent medial clavicle. Range of motion is limited in the right arm. What diagnostic studies need to be performed? What treatment is warranted in the emergency department?
Sternoclavicular Joint Dislocations
SCJ injuries are generally rare. However, due to the increasing amount of contact sports being played, emergency physicians must be aware of how to diagnose and treat these injuries.
The SCJ serves as an important fulcrum for movement of the shoulder girdle. It is the only true articular attachment of the upper extremity to the axial skeleton. Dislocations account for only 3% of all dislocations around the shoulder [1].
Anatomy
The clavicle is the first bone to ossify, but the medial physis is the last fuse, typically between the ages of 23-25 years of age [1]. The medial clavicle sits in a shallow, saddle joint with the superomedial manubrium. The joint requires the subclavius muscle and four separate ligaments for stability [2]. There is an intraarticular fibrocartilanginous disc between the clavicle and the manubrium, which is analogous to the meniscus of the knee [1]. Instability of the joint may be acute, recurrent, or persistent. Displacement can be directed in an anterior, posterior, superior, or inferior direction.

Mechanism of Injury
Dislocations typically are the result of a motor vehicle collision or a sports-related injury. Anterior dislocations are more common that posterior dislocations, but the posterior dislocation is the more concerning injury of the two with a mortality of 3-4% [1]. This is true for two reasons [1,3]:
- The force required for a posterior dislocation is 1.5 times that of an anterior dislocation.
- There is a greater chance (about 30%) of damaging underlying structures, including the brachial plexus, vascular structures, trachea, and esophagus.
Anterior dislocations are the result of a force directed on the shoulder while the arm is held in the abducted position. Posterior dislocations can result from two different mechanisms. First, a medially directed force to the shoulder with the arm adducted and flexed can cause a posterior dislocation. Alternatively, a direct blow to the anteromedial aspect of the clavicle can cause a posterior dislocation.
Physical Examination
The examination of the patient with a potential SCJ injury should be completed in the seated or standing position. Supine positioning may exacerbate severe pain, as may arm motion. The patient will have localized pain and swelling to the joint. Many times the arm will be held across the chest to minimize glenohumeral and scapulothoracic movement. Anterior dislocations will often have a prominent lump from the dislocated medial clavicle. Differentiating the anterior SCJ dislocation from a fracture of the medial clavicle can be challenging. A posterior dislocation can be quite subtle. There may be depression over the SCJ. Associated symptoms such as stridor, dysphagia or shortness of breath indicate compression of the trachea or esophagus, requiring urgent reduction.
Diagnostic Imaging
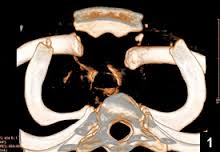
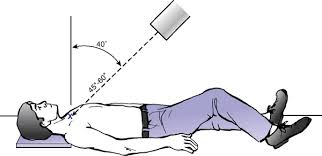
Standard antero-posterior radiographs may be difficulty to interpret due to the confluence of other bony structures. However, a chest x-ray should be performed to exclude other pathology, including pneumothorax, pneumomediastinum, or hemopneumothorax. The addition of the Serendipity view (40 degree cephalic tilt) allows visualization of a SCJ dislocation on plain radiographs [3]. CT has superseded plain films in the diagnosis of SCJ dislocations. CT provides a definitive diagnosis and shows the dislocation in relation to the underlying mediastinal structures.
Treatment
The goals of treatment are:
- Provide adequate pain control
- Reduce or immobilize joint
- Address associated injuries
- Minimize complications
- Arrange appropriate referral
Potential complications of SCJ injuries include:
- Arthritis
- Esophagel injury
- Pneumothorax
- Poor cosmesis
- Vascular injury
- Voice changes
Reduction of dislocations can be done either closed or open. Indications for early surgical intervention include failure of closed reduction and any sign of neurovascular compromise [3].

Closed Reduction Technique of Anterior Dislocation
Acute dislocations (within 7-10 days) are amenable to closed manipulation under procedural sedation in the ED or in the operating room. A bolster should be placed between the scapulae of a supine patient. Traction should be applied to the abducted ipsilateral arm. Pressure is then applied to the medial clavicle. With successful reduction, sling support with scapular protraction should be provided for up to 4 weeks. It is important to remember that there is a greater than 50% rate of repeat dislocation.
Closed Reduction Technique of Posterior Dislocation
Closed reduction of a posterior dislocation is indicated within 10 days of injury. After 10 days, open reduction in the operating room is recommended [1]. There are multiple methods for reducing a posterior dislocation in the literature.
Probably the most well known is the technique of using a towel clip to grasp the medial clavicle and pulling anteriorly until reduction is complete. There is also the abduction-traction technique, where the ipsilateral arm is abducted to ninety degrees and traction is applied. This extension force may translate the medial clavicle anteriorly [1].
Deren et al. described another method which involved extending the ipsilateral arm and abducting it with traction applied. Anterior-posterior pressure is then applied to both shoulders, over the glenohumeral joints [2]. No matter the technique used, a figure of eight splint is recommended for 6 weeks to encourage scapular retraction. Also, some authors recommend that all posterior SCJ dislocations should be admitted for observation, due to the close proximity of vital structures [2].
Case Resolution
You suspect an anterior SCJ dislocation based on the history and physical exam in this football player. You obtain a CT scan of the chest, which confirms the diagnosis. After obtaining consent and under procedural sedation, you easily reduce the dislocation. The patient is placed in a sling and follow up is arranged with orthopedics.
Clinical Bottom Line
Traumatic dislocations of the SCJ are rare, but with increased involvement in contact sports, these injuries will be seen in the ED. Maintain a high clinical suspicion for these injuries, given the proper mechanism. Also be on the look out for associated injuries for posterior dislocations. Reduction can be completed in the ED with subsequent immobilization and orthopedic referral.
References
- Sewell MD et al. Instability of the sternoclavicular joint: current concepts in classification, treatment, and outcomes. Bone Joint J 2013; 95-B: 721-31. PMID: 23723264
- Deren ME et al. Posterior sternoclavicular dislocations: a brief review and technique for closed management of a rare but serious injury. Orthopedic Reviews 2014; 6: 5245. PMID: 24744842
- Balcik BJ et al. Evaluation and treatment of sternoclavicular, clavicular, and acromioclavicular injuries. Prim Care Clin Office Pract 40 (2013): 911-923. PMID: 24209725
Images from:
- healio.com
- wikipedia.org
- msdlatinamerica.com
- drguide.mohp.gov.eg
- boneandjoint.org.uk
Author information

The post Sternoclavicular Joint Dislocations: Diagnosis and Treatment appeared first on ALiEM.