
 Background: Atrial fibrillation and atrial flutter with rapid ventricular rate (AF/AFL with RVR) are the most common subtypes of SVT, comprising a large number of ED visits in aging populations. Currently, rhythm and rate control are the mainstays of therapy in acute settings.
Background: Atrial fibrillation and atrial flutter with rapid ventricular rate (AF/AFL with RVR) are the most common subtypes of SVT, comprising a large number of ED visits in aging populations. Currently, rhythm and rate control are the mainstays of therapy in acute settings.
One common strategy for rate control in stable patients is the use of non-dihydropyridine calcium channel blockers. These agents, verapamil and diltiazem, decrease ventricular rate but also have an effect on vascular smooth muscle, leading to a drop in blood pressure. Hypotension in these patients can complicate management. One proposed method of decreasing the incidence of hypotension when treating Afib or Aflutter is administering IV calcium prior to non-dihydropyridine calcium channel blockers. Currently, the infusion of IV calcium before diltiazem is not well understood, and more studies have focused on administering IV calcium prior to verapamil than diltiazem.
Article: Rossi N et al.. Impact of intravenous calcium with diltiazem for atrial fibrillation/flutter in the emergency department. Am J Emerg Med. 2023. PMID: 36442264
Clinical question: In adult patients with atrial fibrillation and aflutter, what is the effect of calcium and diltiazem on blood pressure compared to diltiazem alone?
What They Did:
- Researchers conducted a multicenter, retrospective cohort study in three community hospitals and two freestanding emergency departments.
- They utilized EMR to gather comprehensive data on patients who received IV calcium and IV diltiazem, or IV diltiazem monotherapy for the treatment of patients with AF/AFL with RVR.
Population:
Inclusion Criteria:
- Patients 18 years old or greater.
- Patients confirmed on ECG to have atrial fibrillation or atrial flutter
- Patients with HR >120 bpm.
- Systolic blood pressure 90 – 140
- Received at least one dose of IV diltiazem
Exclusion Criteria:
- Hemodynamically unstable and require cardioversion
- Prior treatment with another rate control agent (beta-blockers, amiodarone, and digoxin) on the same admission.
- Pregnant or incarcerated patients
- Documentation for systolic BP is incomplete
Intervention:
- Administration of IV calcium within 60 min prior to or 30 min after IV diltiazem administration in patients with AF/AFL with RVR.
Comparator:
- Defined as not having iv calcium administered 120min prior to or 24hrs following the first IV diltiazem administration in patients with atrial fibrillation/atrial flutter with rapid ventricular response.
Outcomes:
Primary outcomes:
- Change in systolic BP within 60 minutes (+/-30) after initial dose of diltiazem is given
Secondary outcomes:
- Time to initial rate control: Defined as HR <100BPM
- Time to sustained rate control: Defined as HR <100 for 3 consecutive hours
- Change in HR in 60 minutes (+/- 30 minutes) after the initial administration of diltiazem
- Hypotension (SBP <90mmHg)
- Bradycardia (HR <50bpm)
- Hypercalcemia (serum calcium >10.5mg/dL)
- Line extravasations within 24 hours
Results:
-
A total of 660 subjects were screened. Of those screened, 198 subjects were in the diltiazem monotherapy group and 56 subjects were in the calcium and diltiazem group.
- 406 subjects were excluded, most commonly 160 were excluded due to inappropriate vital signs (n=160).
-
The diltiazem monotherapy group had a higher median BMI, albumin, and serum calcium
- Weight: 86 KG (Range 68.1 to 106) vs 75.5 KG (Range 60.5 to 104)
-
The diltiazem with calcium group had a higher percentage with chronic kidney disease and malignancy
- CKD: 8.6% vs 21.4%
-
The median baseline systolic blood pressure in the diltiazem with calcium group was significantly lower than the diltiazem monotherapy group.
- SBP: 123mmHg (Range 114 to 132) vs 109mmHg (Range 101 to 121)
- Diltiazem bolus doses were significantly higher in the diltiazem monotherapy group than the diltiazem with calcium group (15mg vs 10mg).
- 10.7% received CaCl
- 89.3% received CaGluc
- Time b/w Ca and Diltiazem: 6.5min (Range 0 to 21min)
Critical Findings
Primary outcome
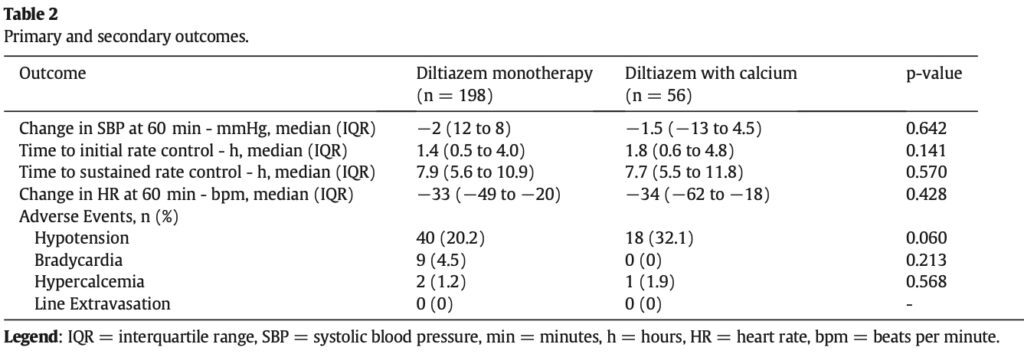
- The change in systolic blood pressure (SBP) 60 minutes (+/- 30 minutes) after initial IV diltiazem administration was similar between the diltiazem monotherapy and diltiazem with calcium groups.
- The median change in SBP for diltiazem monotherapy was -2 mmHg, while for diltiazem with calcium it was -1.5 mmHg.
- The difference in SBP change between the two groups was not statistically significant.
Secondary outcome
- All secondary outcomes were found to be similar (Not statistically significant) between groups (See table above).
- Hypotension occurred more often in the diltiazem with calcium group (20.2% vs 32.1%; P = 0.060)
- Bradycardia occurred more often in the dilitiazem monotherapy group (4.5% vs 0%; P = 0.213)
Strength:
- The multi-center study design increases generalizability of the results.
- Study investigates a clinically important question
- The study population is representative aging population most affected by this disease
- Comprehensive data collection including demographics, medical history, vital signs, laboratory values, and medication details, enabling a thorough analysis of potential confounding factors.
- Largest study to date evaluating the use of IV calcium with diltiazem in the management of AF/AFL with RVR.
- The results of the primary outcome were also validated in the subgroup analysis assessing only those patients that received IV calcium before or at the exact same time as IV diltiazem.
Limitations:
- The primary and secondary outcomes were nearly all disease oriented and not patient oriented.
- Retrospective cohort studies can demonstrate association, but not causation.
- Although the study collected baseline data and demographics, in a non-randomized trial, there may still be unmeasured variables affecting the outcomes.
- The study was dependent on EMR documentation which is prone to error. Critical information such as HR, SBP, drug administration times were occasionally missing.
- Investigators estimated a total of 264 patients (198 in diltiazem monotherapy group and 66 in diltiazem with calcium group) required to find a ≥5mmHg difference in SBP to achieve a power of 80%.
- The investigators screened more than 600 patients but only included 56 subjects in the IV diltiazem with calcium group. The small sample size reduces the statistical power and limits generalizability.
- Investigators enrollend 660 patients in 9 years in 5 EDs; or approximately 6 patients per month; or 1 patient per /month for each ED. They enrolled cohort is likely a convenience sample.
- The baseline characteristics of the two groups slightly differed, with respect to body mass index (BMI), past medical history, laboratory values, SBP, and initial diltiazem bolus dose. These differences could confound the results and affect the interpretation of the findings.
- The treating physicians opted for a fixed dose approach for diltiazem instead of weight-based dosing, resulting in the use of lower-than-recommended doses for treatment.
- The paper does not include information about any interventions administered apart from calcium or diltiazem.
- The primary purpose of Table 1 is to provide a summary of baseline characteristics and demographics of the study population, presenting data in a clear and organized manner. The inclusion of p-values in Table 1 might lead to misinterpretation or improper use of statistical significance.
- 90% of patients got CaGluc which has far less elemental calcium than CaCl. Would a higher dose of elemental calcium made a difference?
- The choice of a 60-minute (+/- 30 minutes) timeframe as the primary outcome is flawed for diltiazem, considering its typical onset of action within 3 minutes and maximum reduction in heart rate occurring between 2 to 7 minutes.
Discussion:
-
Know whats in the calcium you are giving:
- 1g of 10% (100mg/ml) CaGluc = 93mg of elemental calcium
- 1g of 10% (100mg/mL) CaCl = 270mg of elemental calcium
- Essentially 3 ampules of CaGluc = 1 ampule of CaCl
-
Baseline characteristics differed between these groups:
- These differences in baseline characteristics may introduce confounding factors or biases that could affect the study results.
- For example, the lower baseline SBP in the diltiazem with calcium group may have influenced the decision to use calcium in addition to diltiazem and to administer lower initial diltiazem bolus doses.
- These differences could impact the outcomes and adverse events observed in each group.
-
Fixed dosing vs weight-based of diltiazem:
- Anecdotally, we frequently use fixed dosing in the ED for various reasons: the emergent nature of the patient’s condition, challenges in weighing a patient with abnormal vital signs, and patients’ inaccurate recollection of their weight. However, weight-based dosing of diltiazem would have resulted in the administration of higher doses. Perhaps higher doses would have uncovered a statistically significant difference between the two groups.
-
Co-intervention bias:
- Co-Intervention bias refers to a potential bias in clinical trials when additional treatments or interventions are given alongside the primary intervention being studied. This bias occurs when the effects of these additional treatments or interventions interfere with the measured outcomes, making it difficult to separate the true effects of the primary intervention. As a result, co-intervention bias can undermine the internal validity of a study, leading to inaccurate or misleading results.
- For instance, the administration of IV fluids, a commonly used co-intervention alongside diltiazem, has the potential to affect the outcomes examined in the study.
Author’s Conclusion: “In the setting of AF/AFL with RVR, administration of IV calcium with IV diltiazem did not show a significant impact on clinical or safety outcomes compared to IV diltiazem monotherapy.”
Our Conclusion:
The study failed to provide conclusive evidence regarding the effects of IV calcium when used in conjunction with diltiazem for the primary outcome of SBP change and the secondary outcomes of time to rate control, change in HR, and the incidence of hypotension and bradycardia. Several factors, such as the lack of information on the fluids administered in each group, notable baseline differences between groups, and a flawed choice of primary outcome, make it challenging to draw definitive conclusions from this study. Therefore, to establish a more reliable assessment of the potential benefits of calcium supplementation in diltiazem monotherapy for managing AF/AFL, it would be prudent to conduct a multicenter randomized controlled trial with improved design and methodology.
Guest Post By:

Dazi Irving, MD
PGY-1, Emergency Medicine Resident
Vassar Brothers Hospital, Poughkeepsie, New York
E-mail: dazi.irving@nuvancehealth.org
Marco Propersi, DO FAAEM
Vice-Chair, Emergency Medicine
Assistant Emergency Medicine Program Director
Vassar Brothers Hospital, Poughkeepsie, New York
Twitter: @marco_propersi
Post-Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
The post The Concomitant Use of Calcium and Diltiazem for Rapid Atrial Fibrillation appeared first on REBEL EM - Emergency Medicine Blog.